

Tumefactive Multiple Sclerosis Variants: Report of Two Cases of Schilder and Balo Diseases
- PMID: 28698732
- PMCID: PMC5493834
Tumefactive Multiple Sclerosis Variants: Report of Two Cases of Schilder and Balo Diseases
Abstract
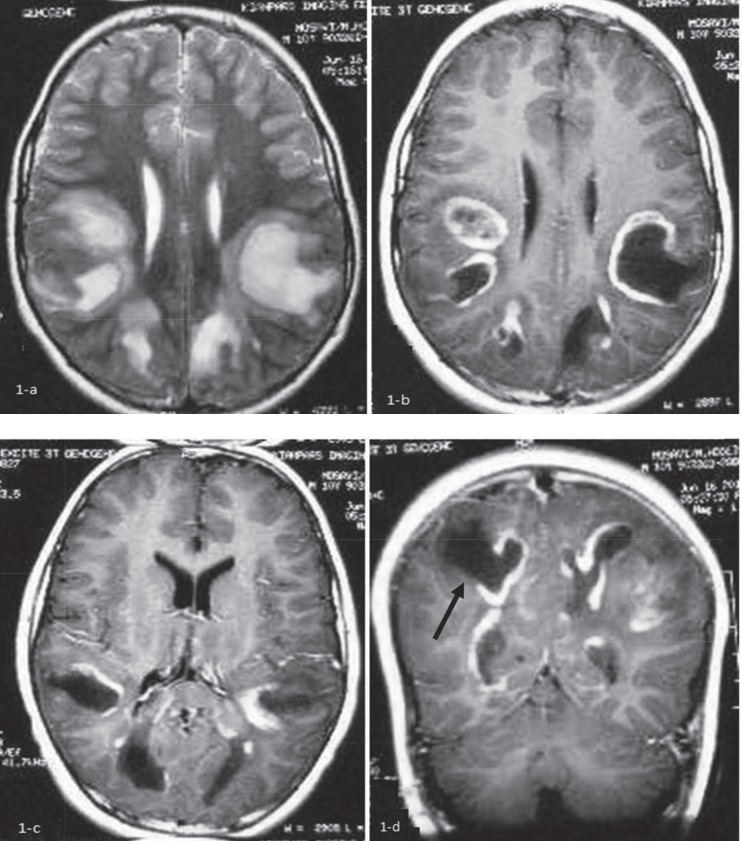
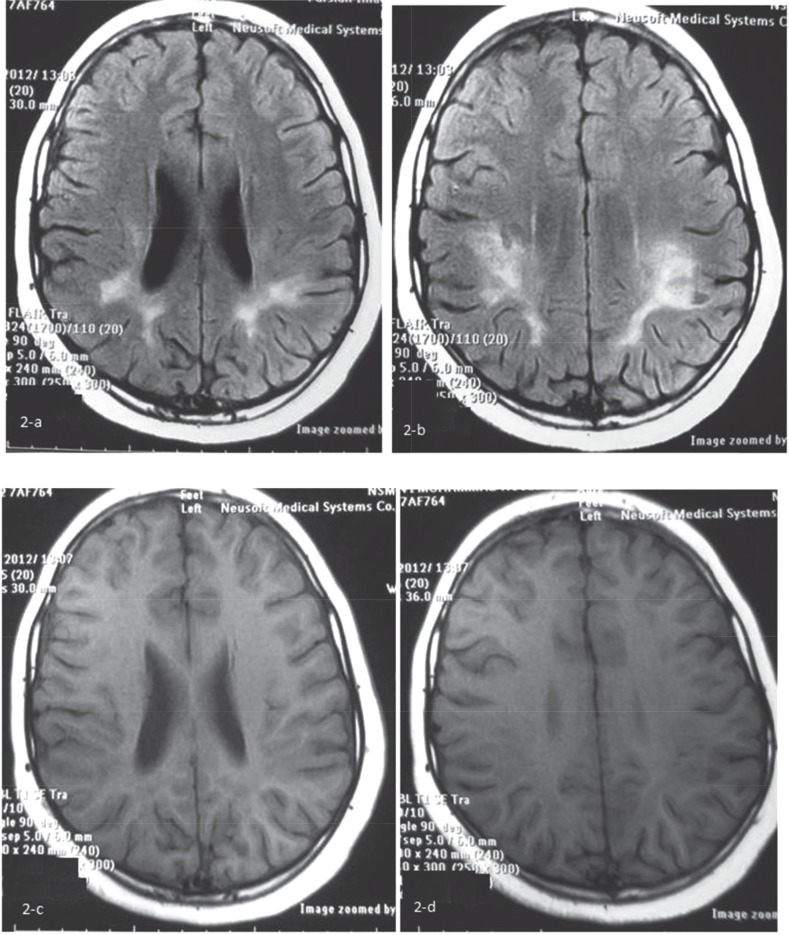
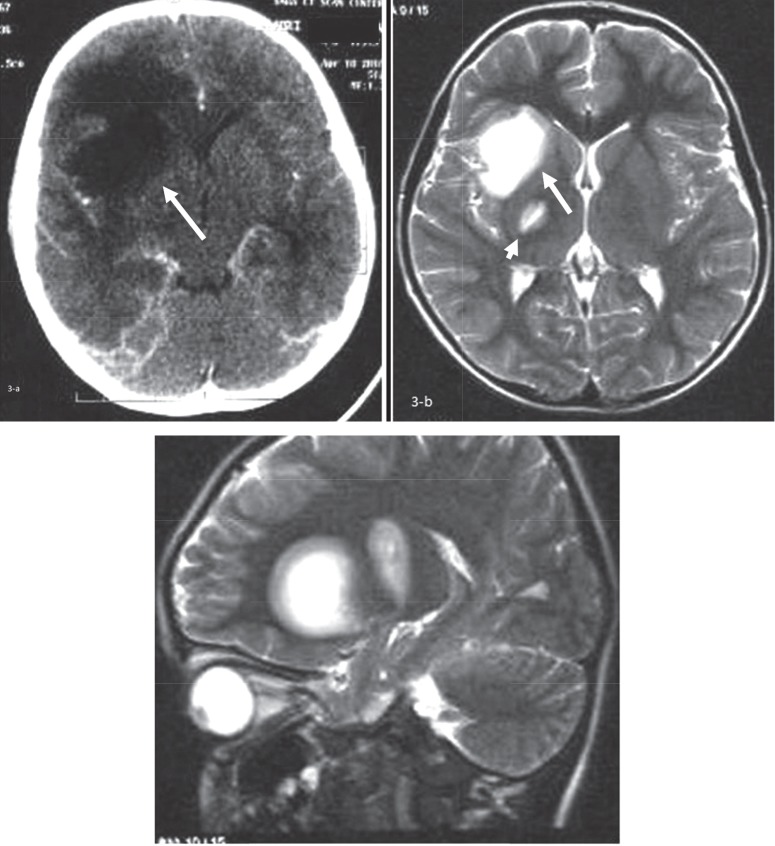
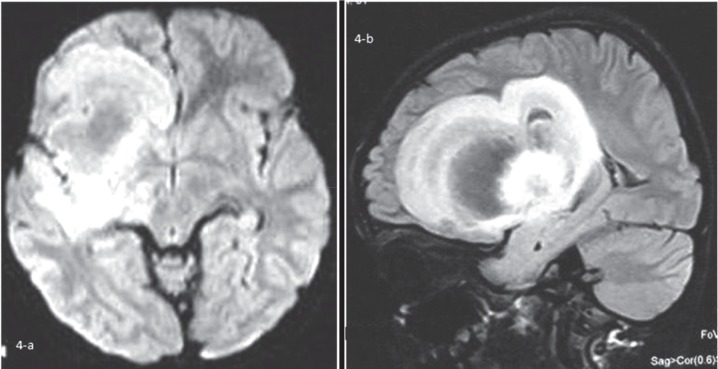
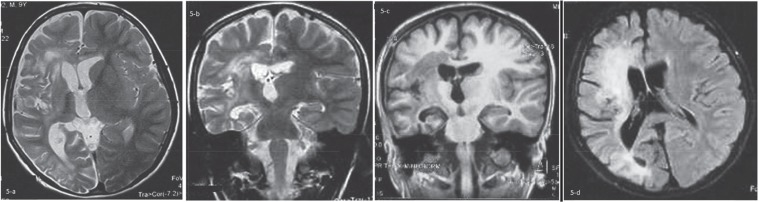
A tumefactive lesion of central nervous system (CNS) is defined as a mass-like lesion with a size greater than 2 cm in brain detected by magnetic resonance imaging (MRI). Neuroimaging may help to distinguish the nature of a tumefactive lesion and therefore, can prevent an unnecessary brain biopsy. Here we emphasized on determining the nature of a CNS tumefactive lesions with the help of MRI and more explanations about demyelinating lesions with focus on Schilder and Balo diseases as two multiple sclerosis variants. We have reported here two boys of 10 and 8 years of age respectively of multiple sclerosis (MS) variants who presented with acute neurologic complications to our hospital as one of the two referral children hospital in Tehran, Iran. Tumefactive demyelinating lesions can be considered a separate entity that itself can contain Schilder disease, Balo disease, some cases of acute disseminated encephalomyelitis (ADEM) or classic MS. MRI can help to establish a diagnosis of a tumefactive lesion and to differentiate among different underlying etiologies.
Keywords: Balo Disease; Central Nervous System; Demyelination; Multiple Sclerosis Variants; Schilder Disease; Tumefactive Lesion.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
References
-
- Bastianello S, Pichiecchio A, Spadaro M, Bergamaschi R, Bramanti P, Colonnese C, et al. Atypical multiple sclerosis: MRI findings and differential diagnosis. Neurol Sci. 2004;25(4):S356–60. - PubMed
-
- Hinnell CJ, Lu JQ, Rajapakse T, Mah JK. Acute tumefactive inflammatory demyelination in a child. Pediatr Neurol. 2011;44:394–5. - PubMed
-
- Legido A, Tenembaum SN, Katsetos CD, Menkes JH. In: Autoimmune and postinfectious disease. 7th ed. Menkes JS, Sarnat HB, Maraia, BL, editors. Philadephia: Lippincott Williams &Wilkins; 2006. pp. 557–634.
-
- Bacigaluppi S, Polonara G, Zavanone ML, Campanella R, Branca V, Gaini SM, et al. Schilder’s disease: noninvasive diagnosis? A case report and review. Neurol Sci. 2009 30:421–30. - PubMed
-
- Fitzgerald MJ, Coleman LT. Recurrent myelinoclastic diffuse sclerosis: a case report of a child with Schilder’s variant of multiple sclerosis. Pediatr Radiol. 2000;30:861Ni. - PubMed
Publication types
LinkOut - more resources
Full Text Sources