Diagnostic approaches for inherited hemolytic anemia in the genetic era
- PMID: 28698843
- PMCID: PMC5503903
- DOI: 10.5045/br.2017.52.2.84
Diagnostic approaches for inherited hemolytic anemia in the genetic era
Abstract
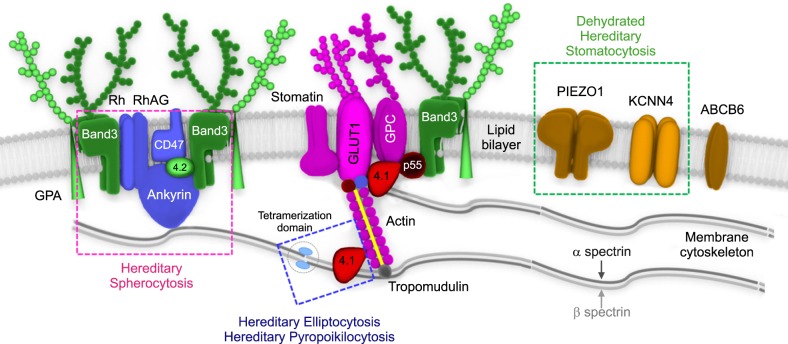
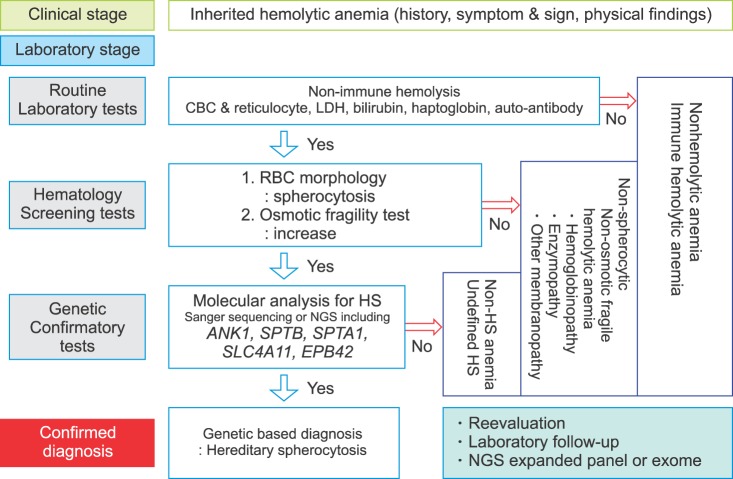
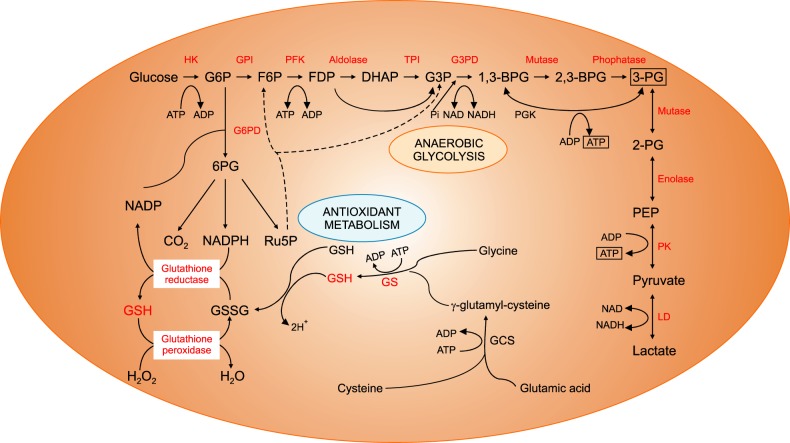
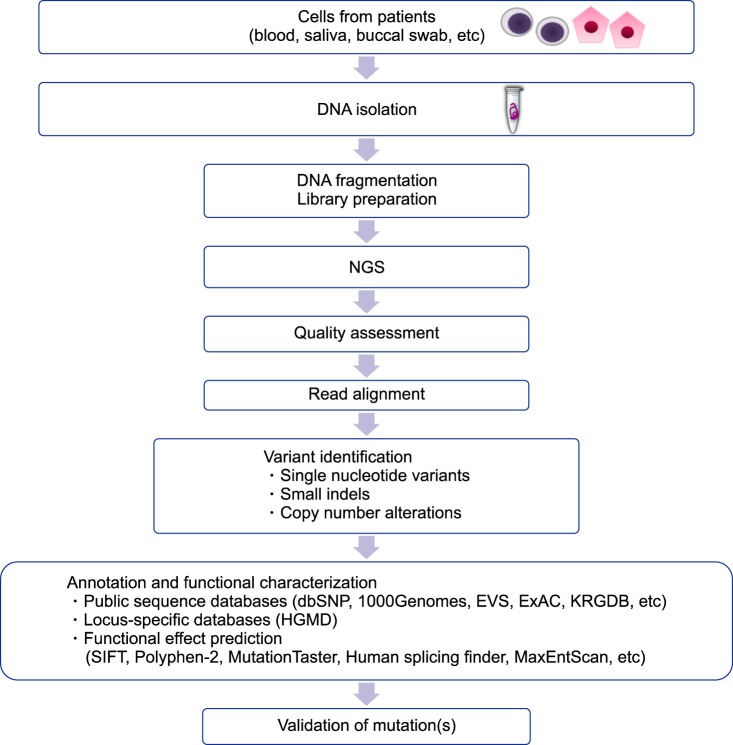
Inherited hemolytic anemias (IHAs) are genetic diseases that present with anemia due to the increased destruction of circulating abnormal RBCs. The RBC abnormalities are classified into the three major disorders of membranopathies, hemoglobinopathies, and enzymopathies. Traditional diagnosis of IHA has been performed via a step-wise process combining clinical and laboratory findings. Nowadays, the etiology of IHA accounts for germline mutations of the responsible genes coding for the structural components of RBCs. Recent advances in molecular technologies, including next-generation sequencing, inspire us to apply these technologies as a first-line approach for the identification of potential mutations and to determine the novel causative genes in patients with IHAs. We herein review the concept and strategy for the genetic diagnosis of IHAs and provide an overview of the preparations for clinical applications of the new molecular technologies.
Keywords: Genetic testing; Inherited hemolytic anemia; Next-generation sequencing.
Conflict of interest statement
Authors' Disclosures of Potential Conflicts of Interest: No potential conflicts of interest relevant to this article were reported.
Figures
Similar articles
-
[Genetic diagnosis for congenital hemolytic anemia].Rinsho Ketsueki. 2016;57(10):1908-1912. doi: 10.11406/rinketsu.57.1908. Rinsho Ketsueki. 2016. PMID: 27725587 Japanese.
-
Establishing the Approach to the Diagnosis of Hemolytic Anemia in the Genetic Era: A Case Series.Cureus. 2024 Aug 27;16(8):e67952. doi: 10.7759/cureus.67952. eCollection 2024 Aug. Cureus. 2024. PMID: 39328644 Free PMC article.
-
Diagnostic yield of targeted next-generation sequencing for pediatric hereditary hemolytic anemia.BMC Med Genomics. 2023 Sep 11;16(1):215. doi: 10.1186/s12920-023-01648-y. BMC Med Genomics. 2023. PMID: 37697358 Free PMC article.
-
Rare Hereditary Hemolytic Anemias: Diagnostic Approach and Considerations in Management.Hematol Oncol Clin North Am. 2019 Jun;33(3):373-392. doi: 10.1016/j.hoc.2019.01.002. Epub 2019 Mar 29. Hematol Oncol Clin North Am. 2019. PMID: 31030808 Review.
-
Laboratory Approach to Hemolytic Anemia.Indian J Pediatr. 2020 Jan;87(1):66-74. doi: 10.1007/s12098-019-03119-8. Epub 2019 Dec 10. Indian J Pediatr. 2020. PMID: 31823208 Review.
Cited by
-
Compound Heterozygosity for KLF1 Mutations Causing Hemolytic Anemia in Children: A Case Report and Literature Review.Front Genet. 2021 Jun 25;12:691461. doi: 10.3389/fgene.2021.691461. eCollection 2021. Front Genet. 2021. PMID: 34249106 Free PMC article.
-
Whole genome sequences discriminate hereditary hemorrhagic telangiectasia phenotypes by non-HHT deleterious DNA variation.Blood Adv. 2022 Jul 12;6(13):3956-3969. doi: 10.1182/bloodadvances.2022007136. Blood Adv. 2022. PMID: 35316832 Free PMC article.
-
Effect of Chinese Herbal Medicine Therapy on Risks of Overall, Diabetes-Related, and Cardiovascular Diseases-Related Mortalities in Taiwanese Patients With Hereditary Hemolytic Anemias.Front Pharmacol. 2022 May 30;13:891729. doi: 10.3389/fphar.2022.891729. eCollection 2022. Front Pharmacol. 2022. PMID: 35712707 Free PMC article.
-
Identification and functional analysis of novel SPTB and ANK1 mutations in hereditary spherocytosis patients.Sci Rep. 2024 Nov 9;14(1):27362. doi: 10.1038/s41598-024-78622-w. Sci Rep. 2024. PMID: 39521890 Free PMC article.
-
Case report: Whole-exome sequencing for a hereditary elliptocytosis case with an unexpectedly low HbA1c.Front Med (Lausanne). 2023 Dec 12;10:1301760. doi: 10.3389/fmed.2023.1301760. eCollection 2023. Front Med (Lausanne). 2023. PMID: 38148910 Free PMC article.
References
-
- Haley K. Congenital hemolytic anemia. Med Clin North Am. 2017;101:361–374. - PubMed
-
- Ucar K. Clinical presentation and management of hemolytic anemias. Oncology (Williston Park) 2002;16(9 Suppl 10):163–170. - PubMed
-
- Lode HN, Krings G, Schulze-Neick I, et al. Pulmonary hypertension in a case of Hb-Mainz hemolytic anemia. J Pediatr Hematol Oncol. 2007;29:173–177. - PubMed
-
- Chiu D, Lubin B. Oxidative hemoglobin denaturation and RBC destruction: the effect of heme on red cell membranes. Semin Hematol. 1989;26:128–135. - PubMed
-
- Jacobasch G, Rapoport SM. Hemolytic anemias due to erythrocyte enzyme deficiencies. Mol Aspects Med. 1996;17:143–170. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources