

Current Status and Future Perspective of Stenting for Symptomatic Intracranial Atherosclerotic Disease: A Meta-Analysis
- PMID: 28698870
- PMCID: PMC5494066
- DOI: 10.1155/2017/3258681
Current Status and Future Perspective of Stenting for Symptomatic Intracranial Atherosclerotic Disease: A Meta-Analysis
Abstract
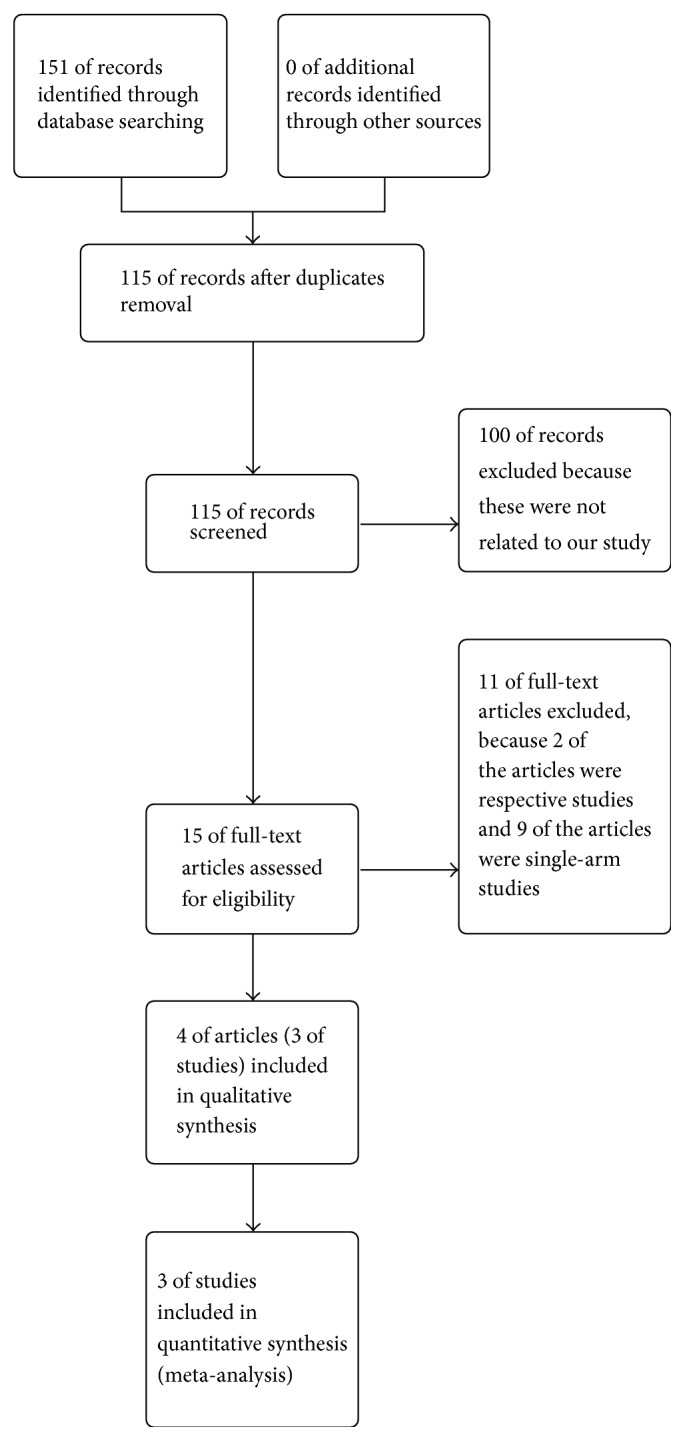
The aim of this study was to evaluate the safety and effectiveness of percutaneous transluminal angioplasty and stenting (PTAS) for intracranial atherosclerotic disease (ICAD) by conducting a meta-analysis. Two independent observers searched PubMed, EMBASE, and Cochrane Library for relevant studies up to 31 December 2016. A meta-analysis was conducted using Review Manager 5.3. Three studies involving 581 cases were included. The meta-analysis indicated that any stroke (RR = 3.13; 95% CI: 1.80-5.42), ischemic stroke (RR = 2.15; 95% CI: 1.19-3.89), and intracranial hemorrhage (RR = 14.71; 95% CI: 1.96-110.48) within 30 days in medical therapy alone were lower compared with PTAS plus medical therapy, but there were no significant differences in any stroke and ischemic stroke beyond 30 days between the two groups. There were also no significant differences in any death and myocardial infarction between the two groups. This meta-analysis demonstrated that, compared with medical therapy alone, PTAS for ICAD had a high risk of complication, but most complications in PTAS group occurred within 30 days after the operation, and beyond 30 days the PTAS was not inferior compared with medical therapy alone. Further studies are needed to reduce the periprocedural complications and reappraise the PTAS.
Figures

















Similar articles
-
Percutaneous transluminal angioplasty and stenting vs aggressive medical management on stroke or intracranial atherosclerotic stenosis: a systematic review and meta-analysis.Sci Rep. 2023 May 9;13(1):7567. doi: 10.1038/s41598-023-34663-1. Sci Rep. 2023. PMID: 37161029 Free PMC article.
-
Percutaneous transluminal angioplasty and stenting for symptomatic intracranial arterial stenosis: a systematic review and meta-analysis.Ther Adv Neurol Disord. 2016 Sep;9(5):351-8. doi: 10.1177/1756285616650357. Epub 2016 May 23. Ther Adv Neurol Disord. 2016. PMID: 27582890 Free PMC article.
-
Stenting versus aggressive medical therapy for intracranial arterial stenosis: more harm than good.Crit Care. 2012 May 9;16(3):310. doi: 10.1186/cc11326. Crit Care. 2012. PMID: 22574950 Free PMC article.
-
CYP2C19 and CES1 polymorphisms and efficacy of clopidogrel and aspirin dual antiplatelet therapy in patients with symptomatic intracranial atherosclerotic disease.J Neurosurg. 2016 Jun;124(6):1746-51. doi: 10.3171/2015.6.JNS15795. Epub 2015 Nov 20. J Neurosurg. 2016. PMID: 26587656 Free PMC article.
-
Percutaneous Transluminal Angioplasty with Stent Placement versus Best Medical Therapy Alone in Symptomatic Intracranial Arterial Stenosis: A Best Evidence Review.Cureus. 2018 Jul 16;10(7):e2988. doi: 10.7759/cureus.2988. Cureus. 2018. PMID: 30397562 Free PMC article. Review.
Cited by
-
Pathological haemodynamics of a middle cerebral artery stenosis validated by computational fluid dynamics.BMJ Case Rep. 2022 Mar 29;15(3):e244519. doi: 10.1136/bcr-2021-244519. BMJ Case Rep. 2022. PMID: 35351770 Free PMC article.
-
Resolute onyx stent more effective than wingspan stent at preventing procedural complications and long-term restenosis.Interv Neuroradiol. 2023 Dec;29(6):691-695. doi: 10.1177/15910199221104633. Epub 2022 May 29. Interv Neuroradiol. 2023. PMID: 35635224 Free PMC article.
-
Stem cell-based therapies for ischemic stroke: a systematic review and meta-analysis of clinical trials.Stem Cell Res Ther. 2020 Jun 26;11(1):252. doi: 10.1186/s13287-020-01762-z. Stem Cell Res Ther. 2020. PMID: 32586371 Free PMC article.
-
Percutaneous transluminal angioplasty and stenting vs aggressive medical management on stroke or intracranial atherosclerotic stenosis: a systematic review and meta-analysis.Sci Rep. 2023 May 9;13(1):7567. doi: 10.1038/s41598-023-34663-1. Sci Rep. 2023. PMID: 37161029 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
