

Is the non-sentinel lymph node compartment the next site for melanoma progression from the sentinel lymph node compartment in the regional nodal basin?
- PMID: 28699042
- PMCID: PMC5884118
- DOI: 10.1007/s10585-017-9854-x
Is the non-sentinel lymph node compartment the next site for melanoma progression from the sentinel lymph node compartment in the regional nodal basin?
Abstract
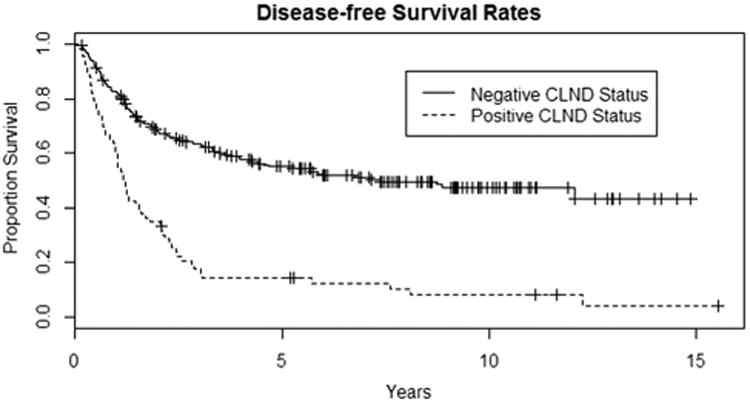
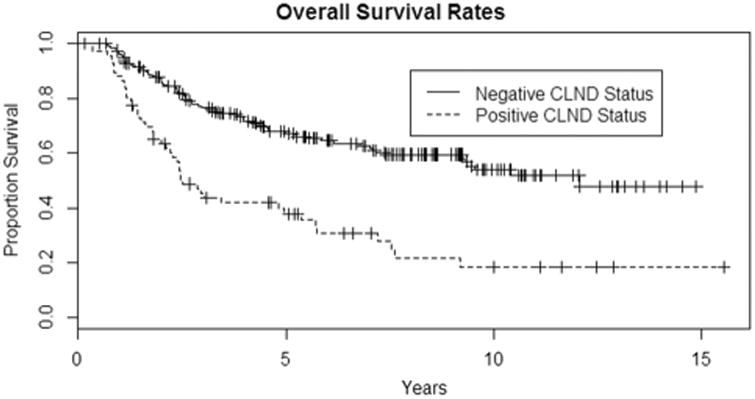
Melanoma patients with additional positive lymph nodes in the completion lymph node dissection (CLND) following a positive sentinel lymph node (SLN) biopsy would have a poorer prognosis than patients with no additional positive lymph nodes. We hypothesize that the progression of disease from the SLN to the non-SLN compartment is orderly and is associated with the worsening of the disease status. Thus, the SLN and non-SLN compartments are biologically different in that cancer cells, in general, arrive in the SLN compartment before spreading to the non-SLN compartment. To validate this concept, we used a large cohort of melanoma patients from our prospective SLN database in an academic tertiary medical center. Adult cutaneous melanoma patients (n = 291) undergoing CLND after a positive SLN biopsy from 1994 to 2009 were analyzed. Comparison of 5-year disease-free survival and 5-year overall survival between positive (n = 66) and negative (n = 225) CLND groups was made. The 5-year disease-free survival rates were 55% (95% CI 49-62%) for patients with no additional LN on CLND versus 14% (95% CI 8-26%) in patients with positive LN on CLND (p < 0.0001, log-rank test). The median disease-free survival time was 7.4 years with negative CLND (95% CI 4.4-15+ years) and 1.2 years with positive CLND (95% CI 1.0-1.8 years). The 5-year overall survival rates were 67% (95% CI 61-74%) for negative CLND versus 38% (95% CI 28-52%) for positive CLND (p < 0.0001, log-rank test). The median overall survival time was 12.1 years for negative CLND (95% CI 9.3-15+ years) and 2.5 years for positive CLND (95% CI 2.2-5.7 years). This study shows that CLND status is a significant prognostic factor for patients with positive SLNs undergoing CLND. Also, it suggests an orderly progression of metastasis from the SLN to the non-SLN compartment. Thus, the SLN in the regional nodal basin draining the primary melanoma may serve as an important gateway for metastasis to the non-SLN compartment and beyond to the systemic sites.
Keywords: Complete lymph node dissection; Cutaneous melanoma; Disease free survival; Overall survival; Sentinel lymph node biopsy.
Figures
References
-
- Morton DL, Wen DR, Wong JH, et al. Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch Surg. 1992;127:392–399. - PubMed
-
- Coit DG, Thompson JA, Andtbacka R, et al. Melanoma, version 4.2014. J Natl Compr Canc Netw. 2014;12:621–629. - PubMed
-
- Han D, Zager JS, Shyr Y, et al. Clinicopathologic predictors of sentinel lymph node metastasis in thin melanoma. J Clin Oncol. 2013;31:4387–4393. - PubMed
-
- Lee JH, Essner R, Torisu-Itakura H, et al. Factors predictive of tumor-positive nonsentinel lymph nodes after tumor-positive sentinel lymph node dissection for melanoma. J Clin Oncol. 2004;22:3677–3684. - PubMed
-
- Murali R, Desilva C, Thompson JF, et al. Non-Sentinel Node Risk Score (N-SNORE): a scoring system for accurately stratifying risk of non-sentinel node positivity in patients with cutaneous melanoma with positive sentinel lymph nodes. J Clin Oncol. 2010;28:4441–4449. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
