

Diagnosis and management of primary aldosteronism
- PMID: 28699986
- PMCID: PMC10118808
- DOI: 10.1590/2359-3997000000274
Diagnosis and management of primary aldosteronism
Abstract
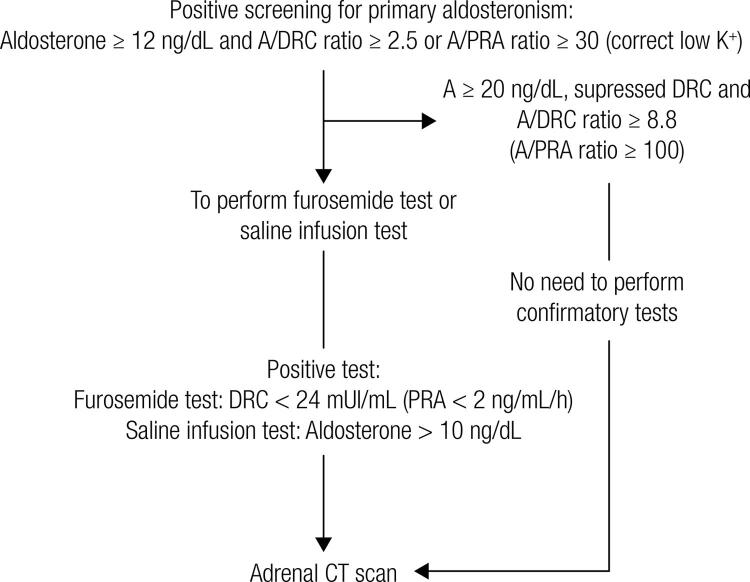
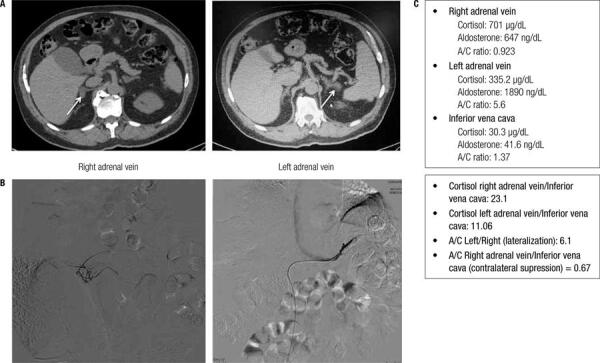
Primary aldosteronism (PA) is the most common form of secondary hypertension (HTN), with an estimated prevalence of 4% of hypertensive patients in primary care and around 10% of referred patients. Patients with PA have higher cardiovascular morbidity and mortality than age- and sex-matched patients with essential HTN and the same degree of blood pressure elevation. PA is characterized by an autonomous aldosterone production causing sodium retention, plasma renin supression, HTN, cardiovascular damage, and increased potassium excretion, leading to variable degrees of hypokalemia. Aldosterone-producing adenomas (APAs) account for around 40% and idiopathic hyperaldosteronism for around 60% of PA cases. The aldosterone-to-renin ratio is the most sensitive screening test for PA. There are several confirmatory tests and the current literature does not identify a "gold standard" confirmatory test for PA. In our institution, we recommend starting case confirmation with the furosemide test. After case confirmation, all patients with PA should undergo adrenal CT as the initial study in subtype testing to exclude adrenocortical carcinoma. Bilateral adrenal vein sampling (AVS) is the gold standard method to define the PA subtype, but it is not indicated in all cases. An experienced radiologist must perform AVS. Unilateral laparoscopic adrenalectomy is the preferential treatment for patients with APAs, and bilateral hyperplasia should be treated with mineralocorticoid antagonist (spironolactone or eplerenone). Cardiovascular morbidity caused by aldosterone excess can be decreased by either unilateral adrenalectomy or mineralocorticoid antagonist. In this review, we address the most relevant issues regarding PA screening, case confirmation, subtype classification, and treatment.
Conflict of interest statement
Disclosure: no potential conflict of interest relevant to this article was reported.
Figures
References
-
- Murray CJ, Lopez AD. Measuring the global burden of disease. N Engl J Med. 2013;369(5):448-57. - PubMed
-
- Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, 1988-2008. JAMA. 2010;303(20):2043-50. - PubMed
-
- Stewart PM. Mineralocorticoid hypertension. Lancet. 1999; 353(9161):1341-7. - PubMed
-
- Lifton RP. Molecular genetics of human blood pressure variation. Science. 1996;272(5262):676-80. - PubMed
-
- Vasan RS, Evans JC, Larson MG, Wilson PW, Meigs JB, Rifai N, et al. Serum aldosterone and the incidence of hypertension in nonhypertensive persons. N Engl J Med. 2004;351(1):33-41. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical