

Application of the SYNTAX score in interventional cardiology: A systematic review and meta-analysis
- PMID: 28700477
- PMCID: PMC5515749
- DOI: 10.1097/MD.0000000000007410
Application of the SYNTAX score in interventional cardiology: A systematic review and meta-analysis
Abstract
Background: Should the SYNTAX score be integrated in Interventional Cardiology? Should it really be considered as a vital decision-making tool in percutaneous coronary intervention (PCI)? To confirm the importance of this score, we aimed to systematically compare the postinterventional adverse cardiovascular outcomes which were observed in patients who were allotted a low versus a high SYNTAX score.
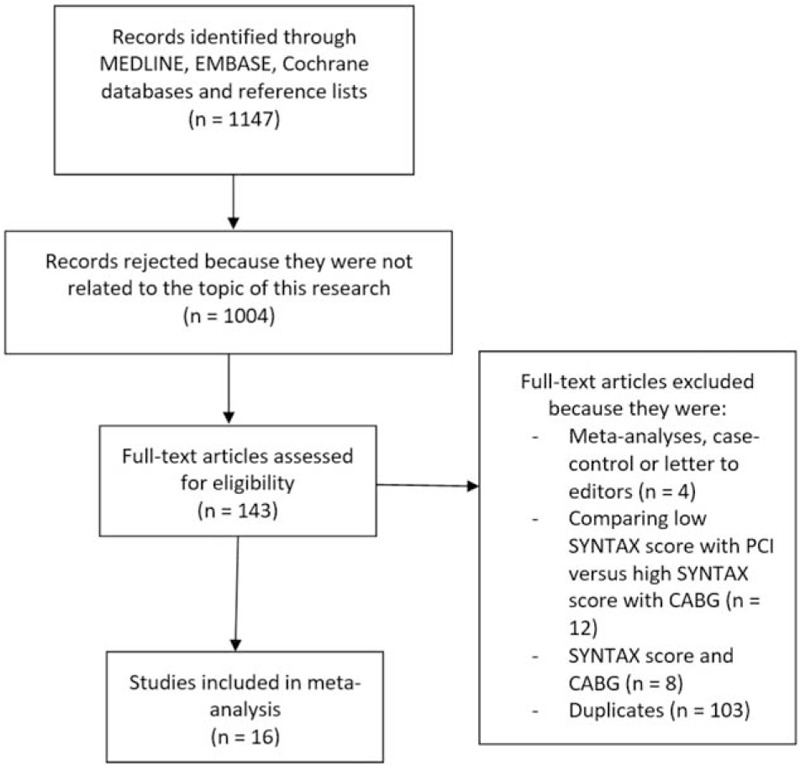
Methods: Randomized controlled trials and observational studies which were published from January 2007 to January 2017 were identified from MEDLINE, EMBASE, and the Cochrane databases using the searched terms 'SYNTAX score and percutaneous coronary intervention.' Adverse cardiovascular outcomes were considered as the major endpoints. Risk ratios (RRs) with 95% confidence intervals (CIs) were used as the statistical parameters, and the main analysis was carried out by the RevMan 5.3 software.
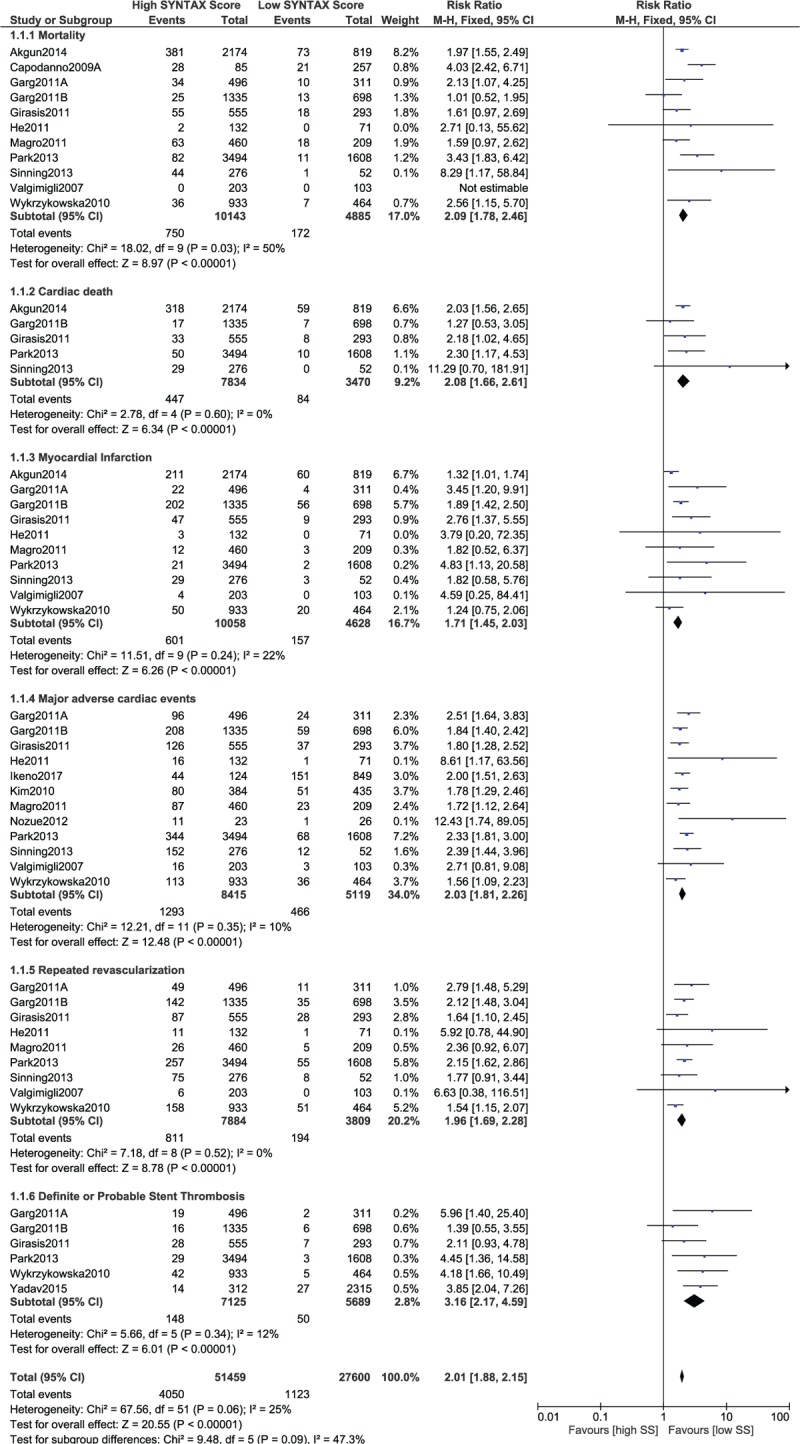
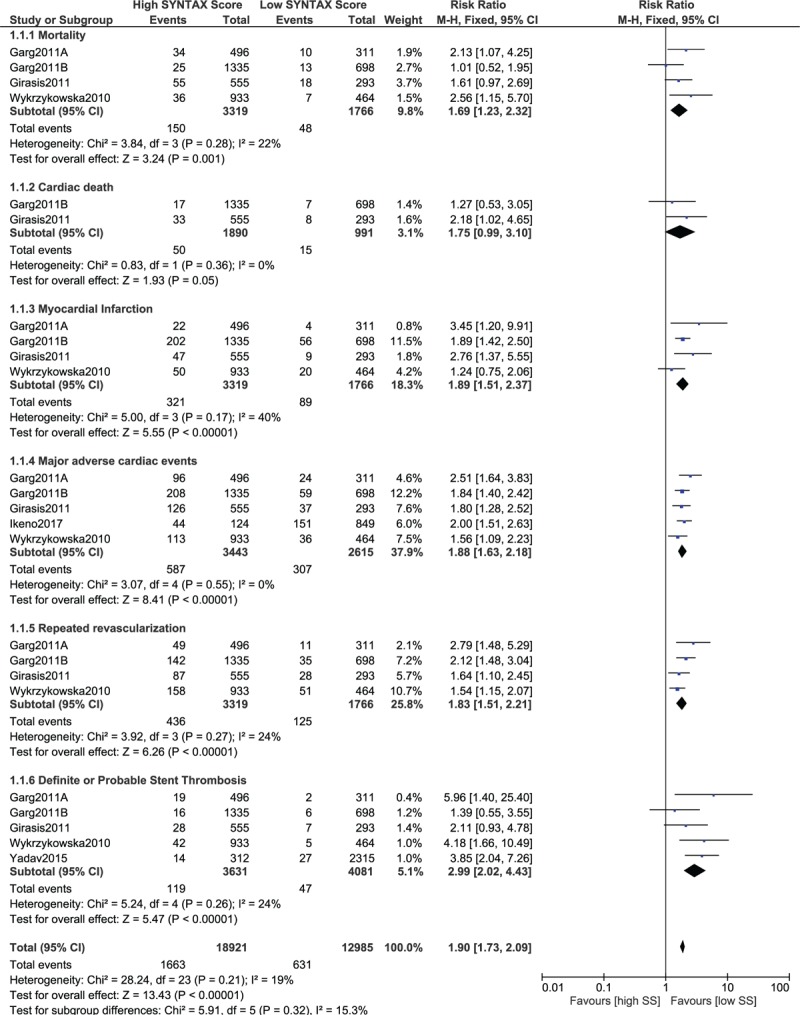
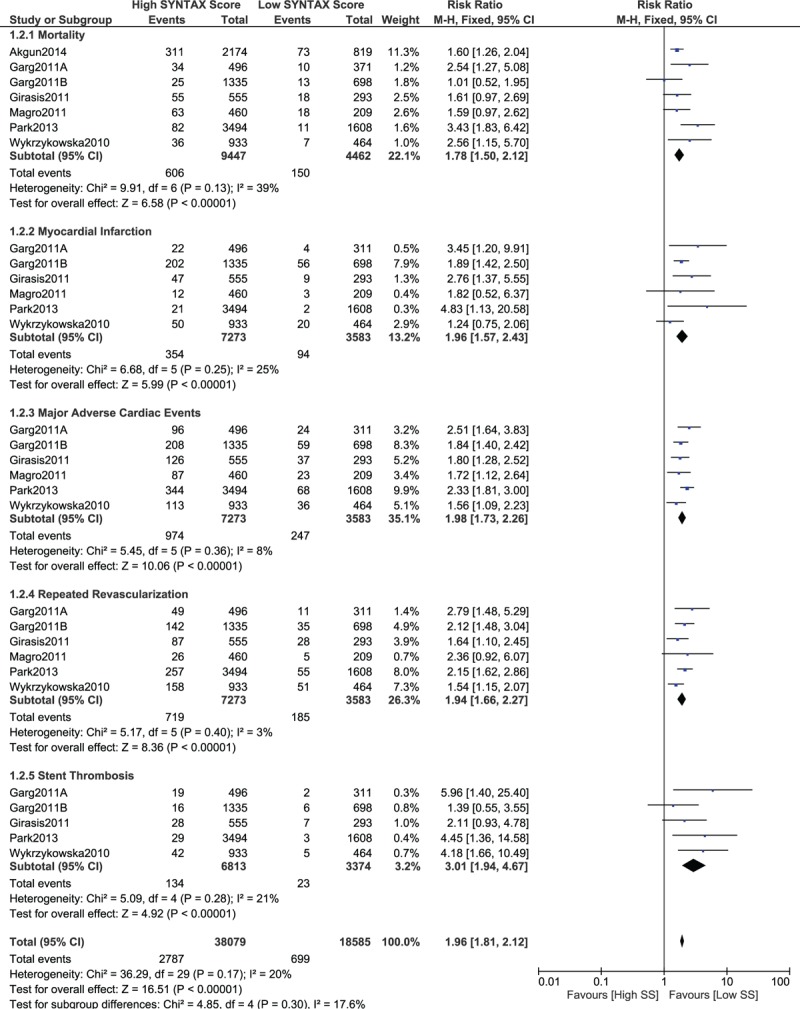
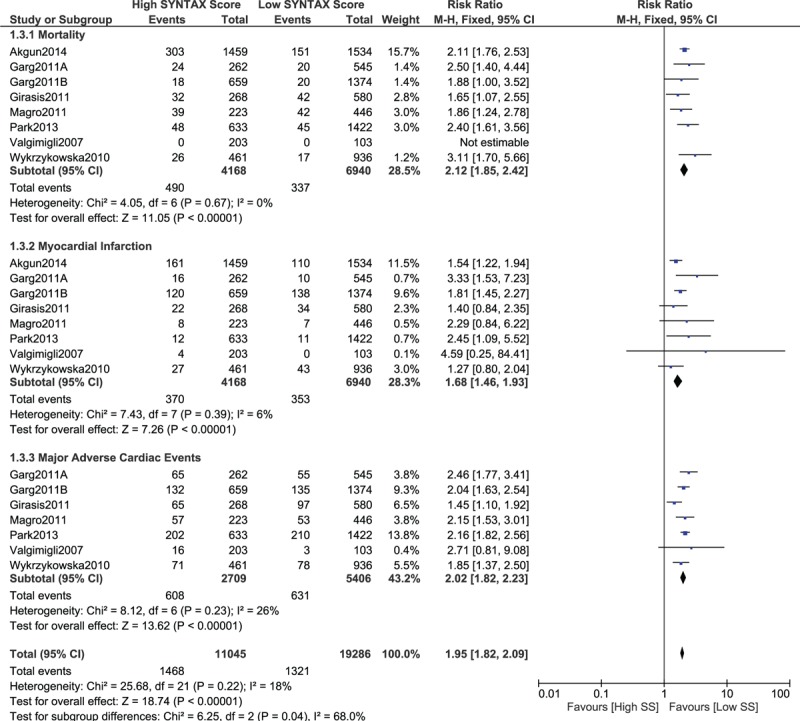
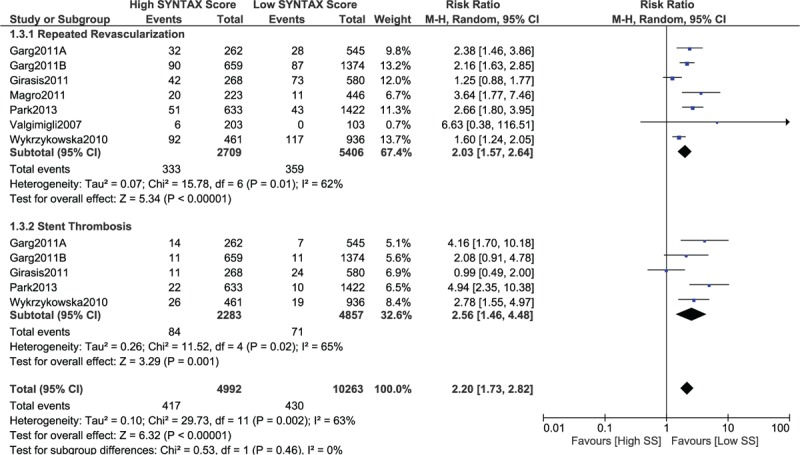
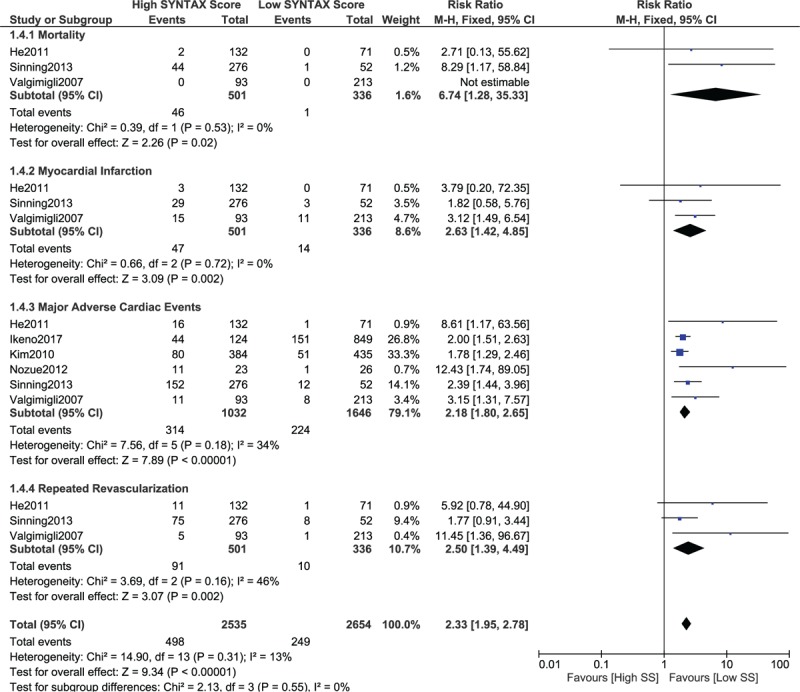
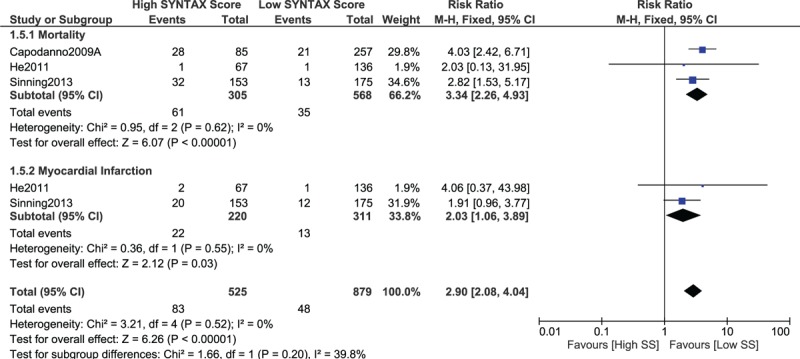
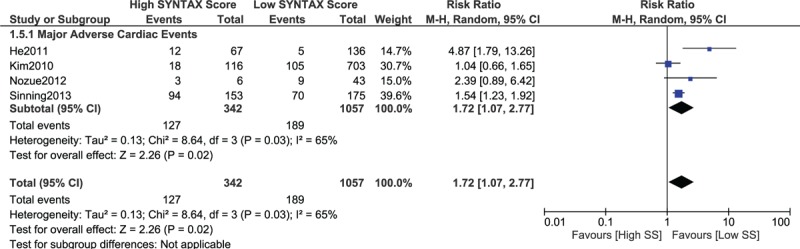
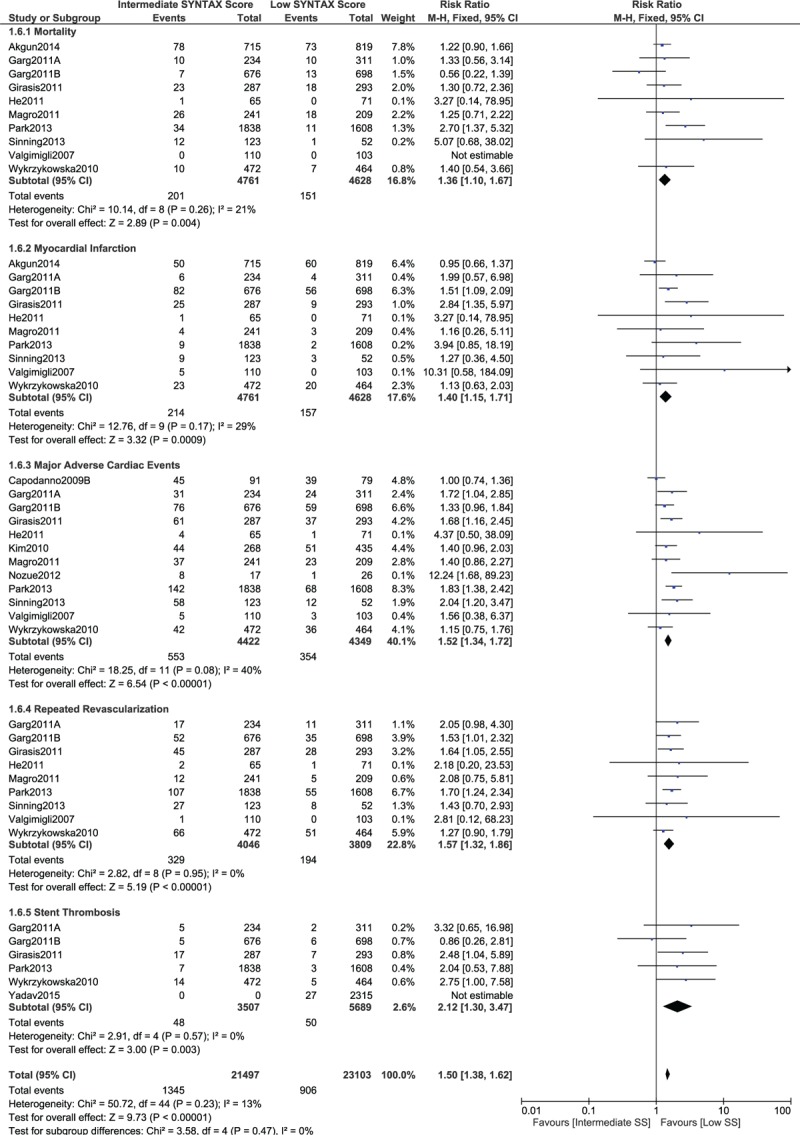
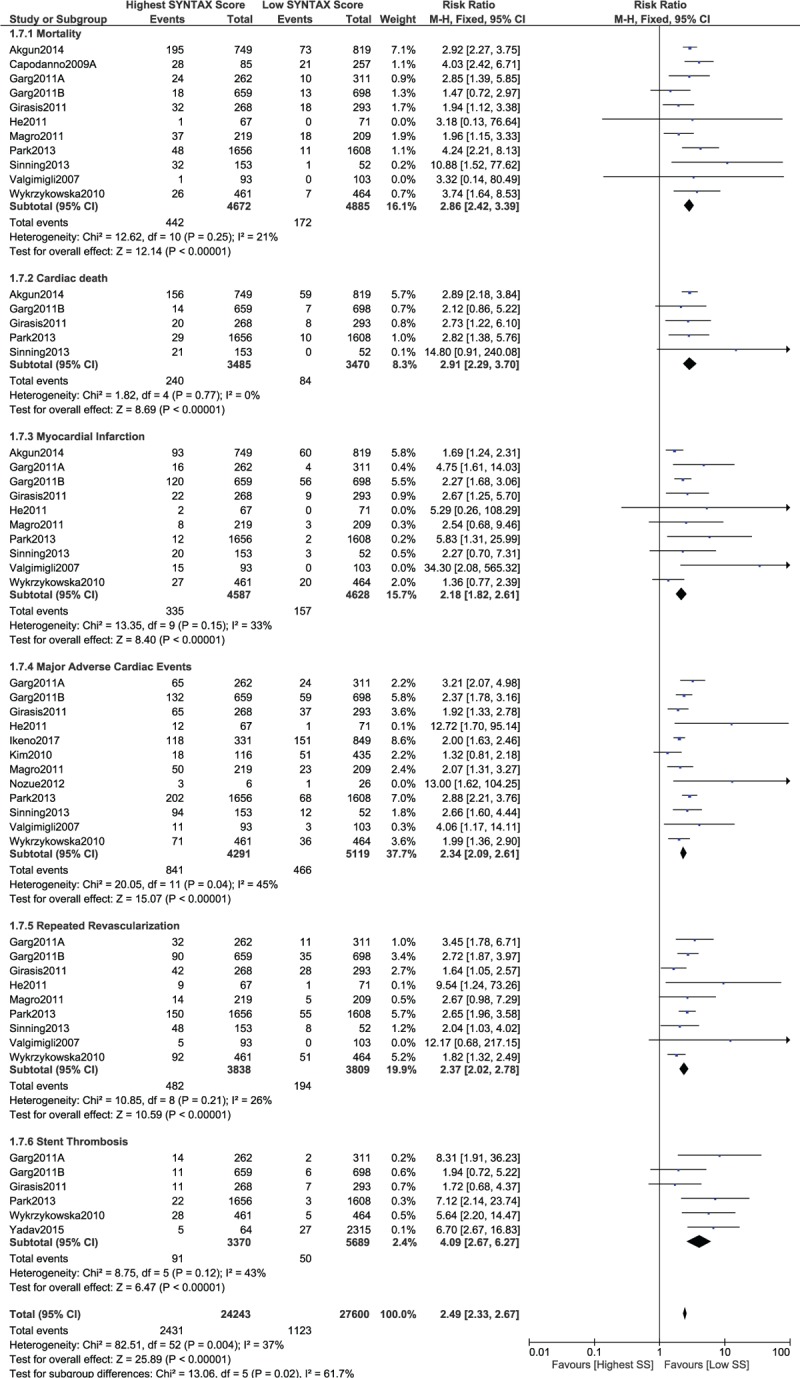
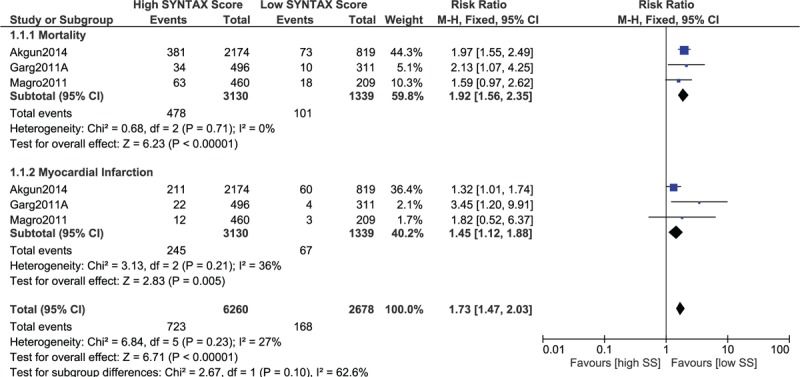
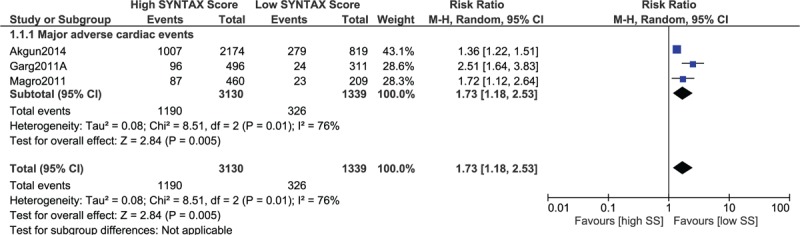
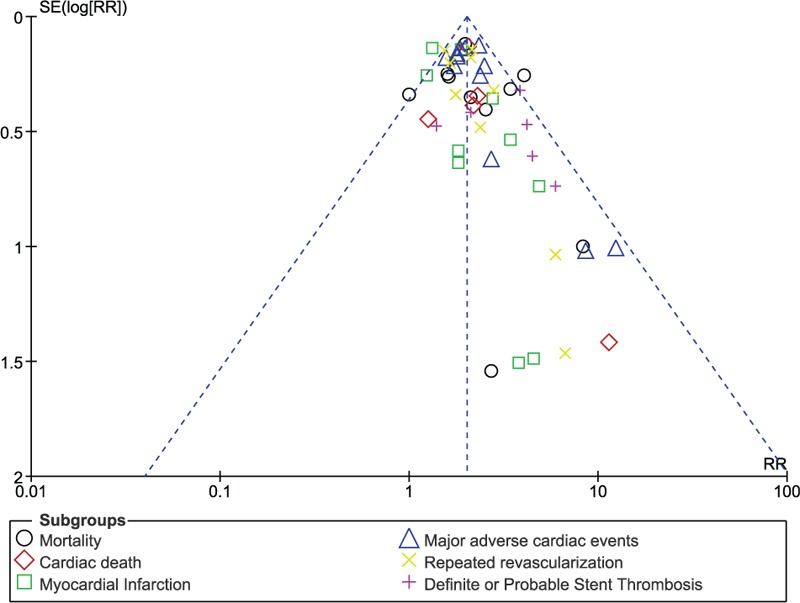
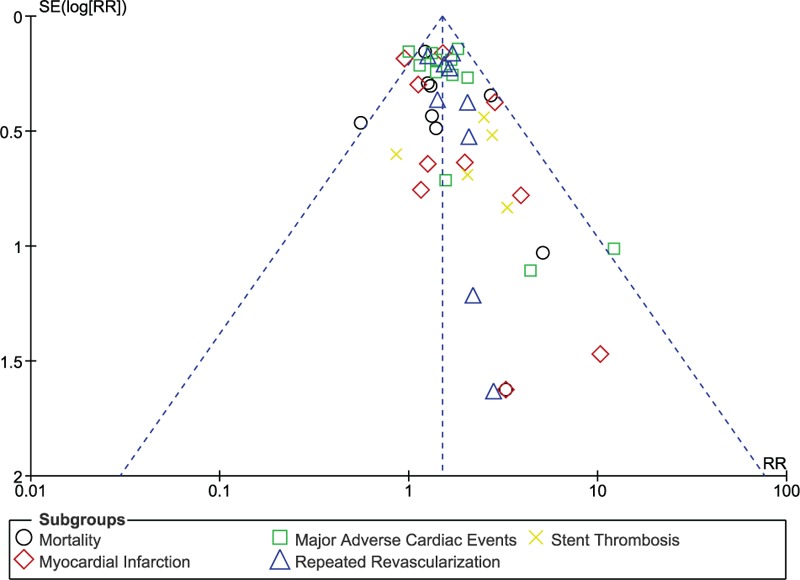
Results: Sixteen studies with a total number of 19,751 participants (8589 participants with a low versus 11,162 participants with a high SYNTAX score) were included. Current results showed mortality to be significantly higher with a higher SYNTAX score (RR 2.09, 95% CI 1.78-2.46, P = .00001). Cardiac death also significantly favored a low SYNTAX score (RR 2.08, 95% CI 1.66-2.61, P = .00001. Similarly, myocardial infarction, major adverse cardiac events, repeated revascularization, and stent thrombosis were significantly higher following a high SYNTAX score (RR 1.71, 95% CI 1.45-2.03, P = .00001; RR 2.03, 95% CI 1.81-2.26, P = .00001; RR 1.96, 95% CI 1.69-2.28, P = .00001; and RR 3.16, 95% CI 2.17-4.59, P = .00001, respectively). Even when patients with ST-segment elevation myocardial infarction were separately analyzed, a low SYNTAX score was still significantly associated with lower adverse outcomes.
Conclusions: This analysis is a confirmatory piece of evidence to show that the application of the SYNTAX score in Interventional Cardiology is apparently relevant. The use of this scoring system to grade patients with coronary artery disease and to further guide for revascularization should be encouraged.
Figures
Similar articles
-
Worse clinical outcomes following percutaneous coronary intervention with a high SYNTAX score: A systematic review and meta-analysis.Medicine (Baltimore). 2017 Jun;96(24):e7140. doi: 10.1097/MD.0000000000007140. Medicine (Baltimore). 2017. PMID: 28614240 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Percutaneous Coronary Intervention, Coronary Artery Bypass Surgery and the SYNTAX score: A systematic review and meta-analysis.Sci Rep. 2017 Mar 2;7:43801. doi: 10.1038/srep43801. Sci Rep. 2017. PMID: 28252019 Free PMC article.
-
Drug-eluting stents versus bare-metal stents for acute coronary syndrome.Cochrane Database Syst Rev. 2017 Aug 23;8(8):CD012481. doi: 10.1002/14651858.CD012481.pub2. Cochrane Database Syst Rev. 2017. PMID: 28832903 Free PMC article.
-
Adverse clinical outcomes associated with a low dose and a high dose of aspirin following percutaneous coronary intervention: a systematic review and meta-analysis.BMC Cardiovasc Disord. 2016 Sep 2;16(1):169. doi: 10.1186/s12872-016-0347-7. BMC Cardiovasc Disord. 2016. PMID: 27590185 Free PMC article.
Cited by
-
The Relationship between Renal Resistive Index and Complexity of Coronary Lesions in Patients with Stable Coronary Artery Diseases.Rev Cardiovasc Med. 2024 May 9;25(5):160. doi: 10.31083/j.rcm2505160. eCollection 2024 May. Rev Cardiovasc Med. 2024. PMID: 39076504 Free PMC article.
-
Redox Status and Telomere-Telomerase System Biomarkers in Patients with Acute Myocardial Infarction Using a Principal Component Analysis: Is There a Link?Int J Mol Sci. 2023 Sep 20;24(18):14308. doi: 10.3390/ijms241814308. Int J Mol Sci. 2023. PMID: 37762611 Free PMC article.
-
Usefulness of white blood cell count to mean platelet volume ratio in the prediction of SYNTAX score in patients with non-ST elevation myocardial infarction.Pak J Med Sci. 2019;35(3):824-829. doi: 10.12669/pjms.35.3.1017. Pak J Med Sci. 2019. PMID: 31258602 Free PMC article.
-
[Complete revascularization with PCI in STEMI patients with multivessel disease, when is the appropriate time?].Arch Cardiol Mex. 2023 Feb 2;93(1):053-061. doi: 10.24875/ACM.21000375. Arch Cardiol Mex. 2023. PMID: 35614449 Free PMC article.
-
Early (≤ 30 Days), Late (31-360 Days) and Very Late (> 360 Days) Stent Thrombosis in Patients with Insulin-Treated versus Non-Insulin-Treated Type 2 Diabetes Mellitus: A Meta-Analysis.Diabetes Ther. 2018 Jun;9(3):1113-1124. doi: 10.1007/s13300-018-0425-1. Epub 2018 Apr 11. Diabetes Ther. 2018. PMID: 29644619 Free PMC article.
References
-
- Lüscher TF. Update on interventional cardiology: outcome according to stent type and implantation technique. Eur Heart J 2016;37:3359–61. - PubMed
-
- Jiménez-Quevedo P, Serrador A, Pérez de Prado A, et al. Spanish Cardiac Catheterization and Coronary Intervention Registry. 25th Official Report of the Spanish Society of Cardiology Working Group on Cardiac Catheterization and Interventional Cardiology (1990-2015). Rev Esp Cardiol (Engl Ed) 2016;69:1180–9. - PubMed
-
- Mehta RM, Agarwal M, Ifedili I, et al. Procedural variations in performing primary percutaneous coronary intervention in patients with ST-elevation myocardial infarction. Curr Probl Cardiol 2017;42:46–60. - PubMed
-
- Faxon DP, Williams DO. Interventional cardiology: current status and future directions in coronary disease and valvular heart disease. Circulation 2016;133:2697–711. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
