

The pharmacological and non-pharmacological treatment of attention deficit hyperactivity disorder in children and adolescents: A systematic review with network meta-analyses of randomised trials
- PMID: 28700715
- PMCID: PMC5507500
- DOI: 10.1371/journal.pone.0180355
The pharmacological and non-pharmacological treatment of attention deficit hyperactivity disorder in children and adolescents: A systematic review with network meta-analyses of randomised trials
Abstract
Background: Attention deficit hyperactivity disorder (ADHD) is one of the most commonly diagnosed psychiatric disorders in childhood. A wide variety of treatments have been used for the management of ADHD. We aimed to compare the efficacy and safety of pharmacological, psychological and complementary and alternative medicine interventions for the treatment of ADHD in children and adolescents.
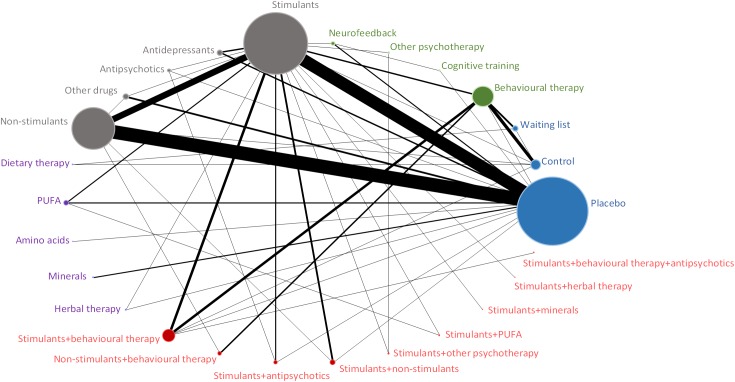
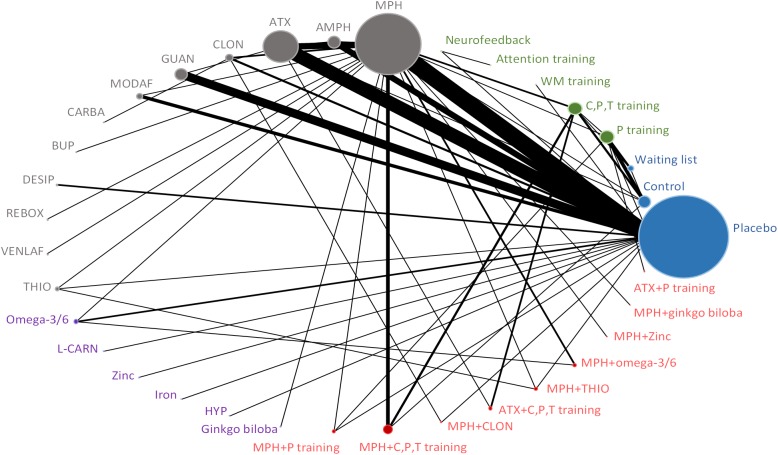
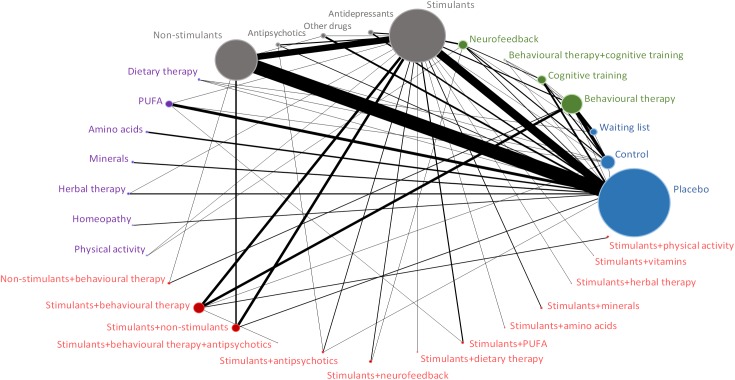
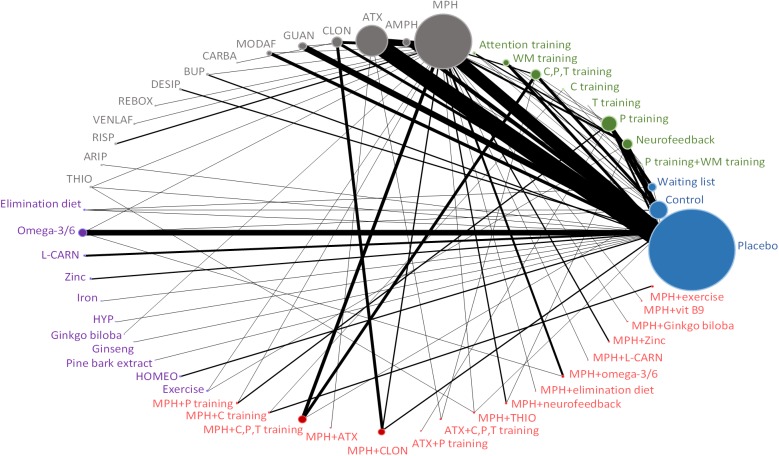
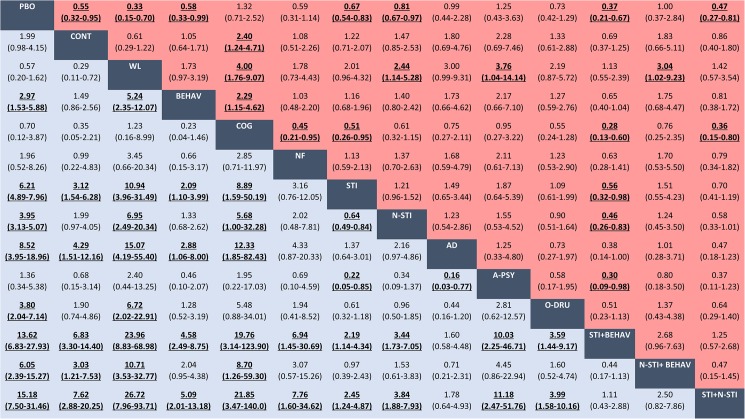
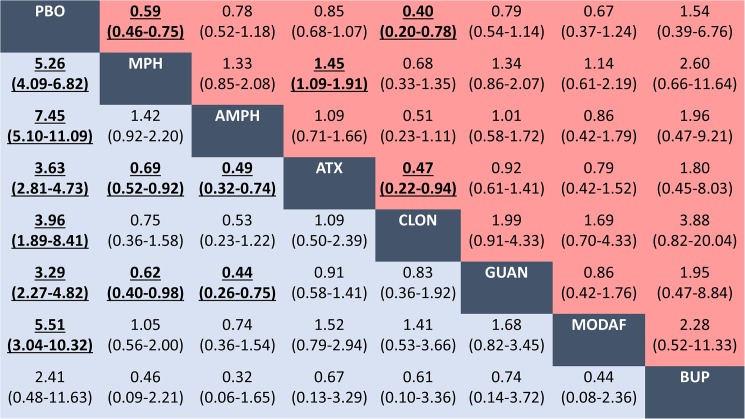
Methods and findings: We performed a systematic review with network meta-analyses. Randomised controlled trials (≥ 3 weeks follow-up) were identified from published and unpublished sources through searches in PubMed and the Cochrane Library (up to April 7, 2016). Interventions of interest were pharmacological (stimulants, non-stimulants, antidepressants, antipsychotics, and other unlicensed drugs), psychological (behavioural, cognitive training and neurofeedback) and complementary and alternative medicine (dietary therapy, fatty acids, amino acids, minerals, herbal therapy, homeopathy, and physical activity). The primary outcomes were efficacy (treatment response) and acceptability (all-cause discontinuation). Secondary outcomes included discontinuation due to adverse events (tolerability), as well as serious adverse events and specific adverse events. Random-effects Bayesian network meta-analyses were conducted to obtain estimates as odds ratios (ORs) with 95% credibility intervals. We analysed interventions by class and individually. 190 randomised trials (52 different interventions grouped in 32 therapeutic classes) that enrolled 26114 participants with ADHD were included in complex networks. At the class level, behavioural therapy (alone or in combination with stimulants), stimulants, and non-stimulant seemed significantly more efficacious than placebo. Behavioural therapy in combination with stimulants seemed superior to stimulants or non-stimulants. Stimulants seemed superior to behavioural therapy, cognitive training and non-stimulants. Behavioural therapy, stimulants and their combination showed the best profile of acceptability. Stimulants and non-stimulants seemed well tolerated. Among medications, methylphenidate, amphetamine, atomoxetine, guanfacine and clonidine seemed significantly more efficacious than placebo. Methylphenidate and amphetamine seemed more efficacious than atomoxetine and guanfacine. Methylphenidate and clonidine seemed better accepted than placebo and atomoxetine. Most of the efficacious pharmacological treatments were associated with harms (anorexia, weight loss and insomnia), but an increased risk of serious adverse events was not observed. There is lack of evidence for cognitive training, neurofeedback, antidepressants, antipsychotics, dietary therapy, fatty acids, and other complementary and alternative medicine. Overall findings were limited by the clinical and methodological heterogeneity, small sample sizes of trials, short-term follow-up, and the absence of high-quality evidence; consequently, results should be interpreted with caution.
Conclusions: Clinical differences may exist between the pharmacological and non-pharmacological treatment used for the management of ADHD. Uncertainties about therapies and the balance between benefits, costs and potential harms should be considered before starting treatment. There is an urgent need for high-quality randomised trials of the multiple treatments for ADHD in children and adolescents. PROSPERO, number CRD42014015008.
Conflict of interest statement
Figures
References
-
- Thomas R, Sanders S, Doust J, Beller E, Glasziou P. Prevalence of attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. Pediatrics. 2015;135(4):e994–1001. doi: 10.1542/peds.2014-3482 - DOI - PubMed
-
- Polanczyk GV, Salum GA, Sugaya LS, Caye A, Rohde LA. Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J Child Psychol Psychiatry. 2015. March;56(3):345–65. doi: 10.1111/jcpp.12381 - DOI - PubMed
-
- GBD 2015 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1603–1658. doi: 10.1016/S0140-6736(16)31460-X - DOI - PMC - PubMed
-
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1545–1602. doi: 10.1016/S0140-6736(16)31678-6 - DOI - PMC - PubMed
-
- Snell T, Knapp M, Healey A, Guglani S, Evans-Lacko S, Fernandez JL, et al. Economic impact of childhood psychiatric disorder on public sector services in Britain: estimates from national survey data. J Child Psychol Psychiatry. 2013;54(9):977–85. doi: 10.1111/jcpp.12055 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
