

Probing for congenital nasolacrimal duct obstruction
- PMID: 28700811
- PMCID: PMC5580992
- DOI: 10.1002/14651858.CD011109.pub2
Probing for congenital nasolacrimal duct obstruction
Abstract
Background: Congenital nasolacrimal duct obstruction (NLDO) is a common condition causing excessive tearing in the first year of life. Infants present with excessive tearing or mucoid discharge from the eyes due to blockage of the nasolacrimal duct system, which can result in maceration of the skin of the eyelids and local infections, such as conjunctivitis, that may require antibiotics. The incidence of nasolacrimal duct obstruction in early childhood ranges from 5% to 20% and often resolves without surgery. Treatment options for this condition are either conservative therapy, including observation (or deferred probing), massage of the lacrimal sac and antibiotics, or probing the nasolacrimal duct to open the membranous obstruction at the distal nasolacrimal duct. Probing may be performed without anesthesia in the office setting or under general anesthesia in the operating room. Probing may serve to resolve the symptoms by opening the membranous obstruction; however, it may not be successful if the obstruction is due to a bony protrusion of the inferior turbinate into the nasolacrimal duct or when the duct is edematous (swollen) due to infection such as dacryocystitis. Additionally, potential complications with probing include creation of a false passage and injury to the nasolacrimal duct, canaliculi and puncta, bleeding, laryngospasm, or aspiration.
Objectives: To assess the effects of probing for congenital nasolacrimal duct obstruction.
Search methods: We searched the Cochrane Central Register of Controlled Trials (CENTRAL), which contains the Cochrane Eyes and Vision Trials Register (2016, Issue 8); MEDLINE Ovid (1946 to 30 August 2016); Embase.com (1947 to 30 August 2016); PubMed (1948 to 30 August 2016); LILACS (Latin American and Caribbean Health Sciences Literature Database; 1982 to 30 August 2016), the metaRegister of Controlled Trials (mRCT) (www.controlled-trials.com), last searched 14 August 2014; ClinicalTrials.gov (www.clinicaltrials.gov), searched 30 August 2016; and the WHO International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/search/en), searched 30 August 2016. We did not use any date or language restrictions in the electronic searches for trials.
Selection criteria: We included randomized controlled trials (RCTs) that compared probing (office-based or hospital-based under general anesthesia) versus no (or deferred) probing or other interventions (observation alone, antibiotic drops only, or antibiotic drops plus massage of the nasolacrimal duct). We did not include studies that compared different probing techniques or probing compared with other surgical procedures. We included studies in children aged three weeks to four years who may have presented with tearing and conjunctivitis.
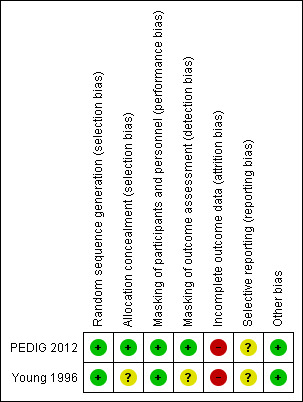
Data collection and analysis: Two review authors independently screened studies for inclusion and independently extracted data and assessed risk of bias for the included studies. We analyzed data using Review Manager software and evaluated the certainty of the evidence using GRADE.
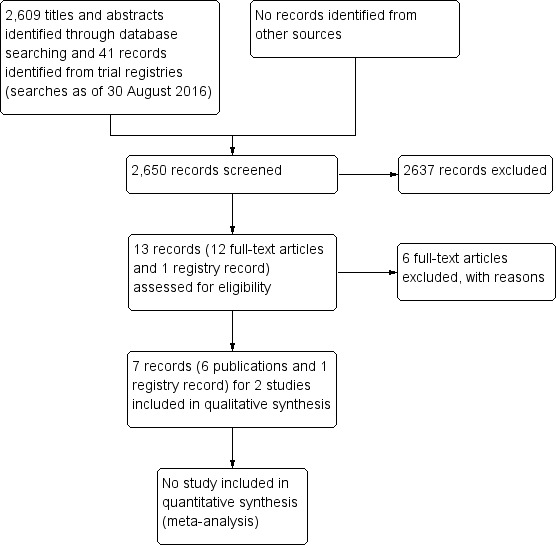
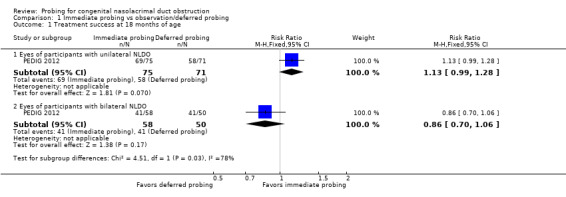
Main results: We identified two RCTs and no ongoing studies; one of the included RCTs was registered. The studies reported on 303 eyes of 242 participants who had unilateral or bilateral congenital nasolacrimal duct obstruction. For both included studies, the interventions compared were immediate office-based probing to remove the duct obstruction versus deferred probing, if needed, after 6 months of observation or once the child reached a certain age.The primary outcome of the review, treatment success at 6 months, was reported partially in one study. Treatment success was not reported at this time point for all children in the immediate probing group; however, 77 of 117 (66%) eyes randomized to deferred probing had resolved without surgery 6 months after randomization and 40 (34%) eyes did not resolve without probing. For children who had unilateral NLDO, those randomized to immediate probing had treatment success more often than those who were randomized to deferred probing (RR 1.41, 95% CI 1.12 to 1.78; 163 children; moderate-certainty evidence). Treatment success for all children was assessed in the study at age 18 months; as an ad hoc analysis in the included study, results were presented separately for children with unilateral and bilateral NLDO (RR 1.13, 95% CI 0.99 to 1.28 and RR 0.86, 95% CI 0.70 to 1.06, respectively; very low-certainty evidence).In the other small study (26 eyes of 22 children), more eyes that received immediate probing were cured within one month after surgery compared with eyes that were randomized to deferred probing and analyzed at age 15 months (RR 2.56, 95% CI 1.16 to 5.64). We considered the evidence to be low-certainty due to imprecision from the small study size and risk of bias concerns due to attrition bias.One study reported on the number of children that required reoperation; however, these data were reported only for immediate probing group. Nine percent of children with unilateral NLDO and 13% with bilateral NLDO required secondary procedures.One study reported cost-effectiveness of immediate probing versus deferred probing. The mean cost of treatment for immediate probing was less than for deferred probing; however, there is uncertainty as to whether there is a true cost difference (mean difference USD -139, 95% CI USD -377 to 94; moderate-certainty evidence).Reported complications of the treatment were not serious. One study reported that there were no complications for any surgery and no serious adverse events, while the other study reported that bleeding from the punctum occurred in 20% of all probings.
Authors' conclusions: The effects and costs of immediate versus deferred probing for NLDO are uncertain. Children who have unilateral NLDO may have better success from immediate office probing, though few children have participated in these trials, and investigators examined outcomes at disparate time points. Determining whether to perform the procedure and its optimal timing will require additional studies with greater power and larger, well-run clinical trials to help our understanding of the comparison.
Conflict of interest statement
None known.
Figures
Update of
References
References to studies included in this review
PEDIG 2012 {published data only}
-
- Lee KA, Chandler DL, Repka MX, Beck RW, Foster NC, Frick KD, et al. A randomized trial comparing cost‐effectiveness of immediate office probing versus observation with deferred facility probing for unilateral congenital nasolacrimal duct obstruction. Journal of AAPOS 2012;16(1):e6.
Young 1996 {published data only}
-
- Young JD, MacEwen CJ, Ogston SA. Congenital nasolacrimal duct obstruction in the second year of life: a multicentre trial of management. Eye 1996;10(4):485‐91. - PubMed
References to studies excluded from this review
Al‐Faky 2015 {published data only}
-
- Al‐Faky YH, Mousa A, Kalantan H, Al‐Otaibi A, Alodan H, Alsuhaibani AH. A prospective, randomised comparison of probing versus bicanalicular silastic intubation for congenital nasolacrimal duct obstruction. British Journal of Ophthalmology 2015;99(2):246‐50. - PubMed
Chaabouni 1993 {published data only}
-
- Chaabouni M, Zayani A, Chebihi S, Guiaa R, Ben HH. Congenital obstruction of lacrimal ducts in 578 children. Archives Françaises de Pédiatrie 1993;50(2):107‐9. - PubMed
Ekinciler 1994 {published data only}
-
- Ekinciler OF, Doğan H, Tatlişen N, Karaküçük S. Congenital nasolacrimal duct obstruction in Kayseri, Turkey. Turkish Journal of Pediatrics 1994;36(1):21‐33. - PubMed
Hernandez 1967 {published data only}
-
- Hernandez JA. Treatment of congenital lacrimal duct obstruction [Actualizacion del tratamiento de la obstruccion congenita de las via lagrimales]. Archivos de Oftalmologia de Buenos Aires 1967;42(4):59‐61. - PubMed
Ishikawa 1990 {published data only}
-
- Ishikawa C, Tanaka H, Toibana M. Early probing for congenital nasolacrimal duct obstruction. Folia Ophthalmologica Japonica 1990;41(5):940‐4.
Robb 1985 {published data only}
-
- Robb RM. Treatment of congenital nasolacrimal system obstruction. Journal of Pediatric Ophthalmology and Strabismus 1985;22(1):36‐7. - PubMed
Additional references
Cassady 1948
-
- Cassady JV. Dacryocystitis of infancy. American Journal of Ophthalmology 1948;31(7):773‐80. - PubMed
Cassady 1952
-
- Cassady JV. Developmental anatomy of nasolacrimal duct. A.M.A. Archives of Ophthalmology 1952;47(2):141‐58. - PubMed
Deeks 2011
-
- Deeks JJ, Higgins JP, Altman DG editor(s). Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JP, Green S editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Ffookes 1962
GRADEpro 2014 [Computer program]
-
- GRADE Working Group, McMaster University. GRADEpro GDT. Version accessed 11 January 2017. Hamilton (ON): GRADE Working Group, McMaster University, 2014.
Guerry 1948
-
- Guerry D, Kendig EL. Congenital impatency of the nasolacrimal duct. Archives of Ophthalmology 1948;39(2):193‐204. - PubMed
Higgins 2011
-
- Higgins JP, Altman DG, Sterne JAC editor(s). Chapter 8: Assessing risk of bias in included studies. In: Higgins JP, Green S editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Lin 2016
-
- Lin AE, Chang YC, Lin MY, Tam KW, Shen YD. Comparison of treatment for congenital nasolacrimal duct obstruction: a systematic review and meta‐analysis. Canadian Journal of Ophthalmology 2016;51(1):34‐40. - PubMed
MacEwen 1991
-
- MacEwen CJ, Young JD. Epiphora during the first year of life. Eye 1991;5(Pt 5):596‐600. - PubMed
Nelson 1985
-
- Nelson LB, Calhoun JH, Menduke H. Medical management of congenital nasolacrimal duct obstruction. Ophthalmology 1985;92(9):1187‐90. - PubMed
Paul 1985
-
- Paul TO. Medical management of congenital nasolacrimal duct obstruction. Journal of Pediatric Ophthalmology and Strabismus 1985;22(2):68‐70. - PubMed
Paul 1994
-
- Paul TO, Shepherd R. Congenital nasolacrimal duct obstruction: natural history and the timing of optimal intervention. Journal of Pediatric Ophthalmology and Strabismus 1994;31(6):362‐7. - PubMed
PEDIG 2008
Petersen 1978
-
- Petersen RA, Robb RM. The natural course of congenital obstruction of the nasolacrimal duct. Journal of Pediatric Ophthalmology and Strabismus 1978;15(4):246‐50. - PubMed
RevMan 2014 [Computer program]
-
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Schnall 2013
-
- Schnall BM. Pediatric nasolacrimal duct obstruction. Current Opinion in Ophthalmology 2013;24(5):421‐4. - PubMed
Sevel 1981
-
- Sevel D. Development and congenital abnormalities of the nasolacrimal apparatus. Journal of Pediatric Ophthalmology and Strabismus 1981;18(5):13‐9. - PubMed
Shekunov 2011
Stager 1992
-
- Stager D, Baker JD, Frey T, Weakley DR, Birch, EE. Office probing of congenital nasolacrimal duct obstruction. Ophthalmic Surgery 1992;23(7):482‐4. - PubMed
Tan 2001
-
- Tan AD, Rubin PA, Sutula FC, Remulla HD. Congenital nasolacrimal duct obstruction. International Ophthalmology Clinics 2001;41(4):57‐69. - PubMed
Wesley 1985
-
- Wesley RE. Inferior turbinate fracture in the treatment of congenital nasolacrimal duct obstruction and congenital nasolacrimal duct anomaly. Ophthalmic Surgery 1985;16(6):368‐71. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials