

The current level of shared decision-making in anesthesiology: an exploratory study
- PMID: 28701156
- PMCID: PMC5508628
- DOI: 10.1186/s12871-017-0386-3
The current level of shared decision-making in anesthesiology: an exploratory study
Abstract
Background: Shared decision-making (SDM) seeks to involve both patients and clinicians in decision-making about possible health management strategies, using patients' preferences and best available evidence. SDM seems readily applicable in anesthesiology. We aimed to determine the current level of SDM among preoperative patients and anesthesiology clinicians.
Methods: We invited 115 consecutive preoperative patients, visiting the pre-assessment outpatient clinic of the department of Anesthesiology at the Academic Medical Center of Amsterdam. Inclusion criteria were patients who needed surgery in the arms, lower abdomen or legs, and in whom three anesthesia techniques were feasible. The SDM-level of the consultation was scored objectively by independent observers who judged audio-recordings of the consultation using the OPTION5-scale, ranging from 0% (no SDM) to 100% (optimum SDM), as well as subjectively by patients (using the SDM-Q-9 and CollaboRATE questionnaires) and clinicians (SDM-Q-Doc questionnaire). Objective and subjective SDM-levels were assessed on five-point and six-point Likert scales, respectively. Both scores were expressed as percentages.
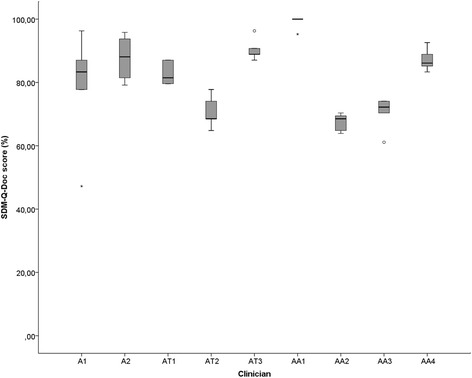
Results: Data of 80 patients could be analysed. Objective SDM-scores were low (30.5%). Subjective scores of the SDM-Q-9 and CollaboRATE were high among patients (91.7% and 96.3%, respectively) and among clinicians (SDM-Q-Doc; 84.3%). Apparently, they appreciated satisfaction rather than SDM, being poorly aware of what SDM entails.
Conclusion: The level of SDM in an outpatient anesthesiology clinic where preoperative patients receive information about various possible anesthesia options, was found to be low. Thus, there is room for improving the level of SDM. Some suggestions are given how this can be achieved.
Keywords: Patient education; Preoperative period; Shared decision-making; Surgical procedures, operative.
Conflict of interest statement
Ethics approval and consent to participate
The hospital’s medical ethics review board approved the study and waived the need for full assessment, because the study did not have a serious impact on patient integrity or their treatment. All patients signed informed consent for participation in this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures




References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
