

The spectrum of mild traumatic brain injury: A review
- PMID: 28701496
- PMCID: PMC5562956
- DOI: 10.1212/WNL.0000000000004214
The spectrum of mild traumatic brain injury: A review
Abstract
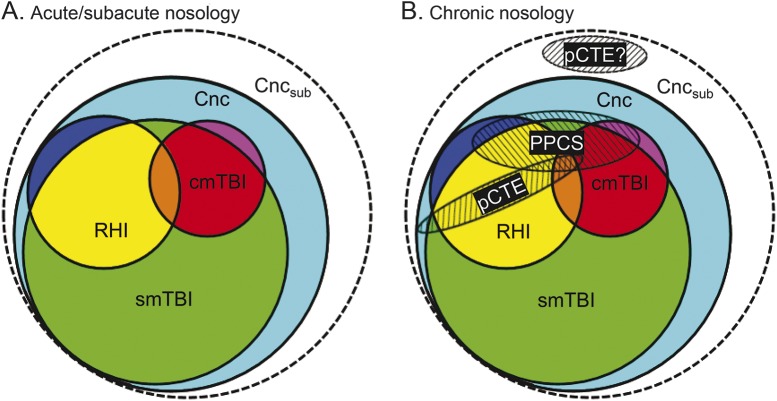
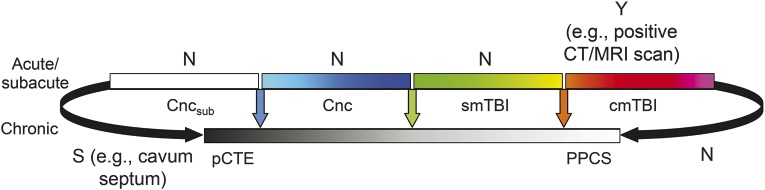
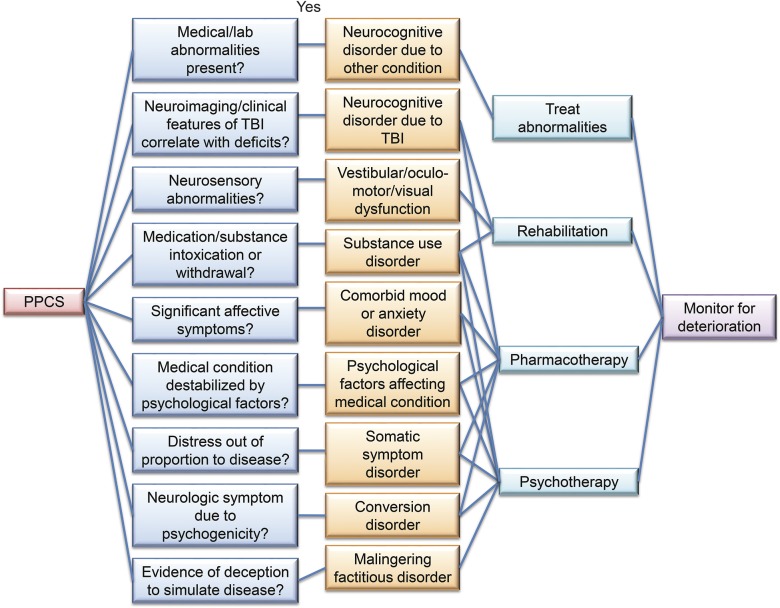
Objective: This review provides an in-depth overview of diagnostic schema and risk factors influencing recovery during the acute, subacute (operationally defined as up to 3 months postinjury), and chronic injury phases across the full spectrum of individuals (e.g., athletes to neurosurgery patients) with mild traumatic brain injury (mTBI). Particular emphasis is placed on the complex differential diagnoses for patients with prolonged postconcussive symptoms.
Methods: Select literature review and synthesis.
Results: In spite of an increase in public awareness surrounding the acute and potential long-term effects of mTBI, the medical field remains fragmented both in terms of the diagnostic (different criteria proffered by multiple medical organizations) and prognostic factors that influence patient care.
Conclusions: Given the lack of objective biomarkers and the spectrum of different disorders that likely encompass mTBI, clinicians are encouraged to adopt a probabilistic, rather than definitive, diagnostic and prognostic framework. The relevance of accurately diagnosing and managing the different manifestations of mTBI becomes clear when one considers the overall incidence of the disorder (42 million people each year worldwide), and the different treatment implications for patients with a true neurodegenerative disorder (e.g., chronic traumatic encephalopathy; rare) vs potentially treatable conditions (e.g., depression or posttraumatic headache; frequent).
© 2017 American Academy of Neurology.
Figures
References
-
- McCrea M, Guskiewicz KM, Marshall SW, et al. . Acute effects and recovery time following concussion in collegiate football players: the NCAA Concussion Study. JAMA 2003;290:2556–2563. - PubMed
-
- Karr JE, Areshenkoff CN, Garcia-Barrera MA. The neuropsychological outcomes of concussion: a systematic review of meta-analyses on the cognitive sequelae of mild traumatic brain injury. Neuropsychology 2014;28:321–336. - PubMed
-
- DeKosky ST, Ikonomovic MD, Gandy S. Traumatic brain injury: football, warfare, and long-term effects. N Engl J Med 2010;363:1293–1296. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical