

Tuberculosis exposure, infection and disease in children: a systematic diagnostic approach
- PMID: 28702302
- PMCID: PMC5471717
- DOI: 10.1186/s41479-016-0023-9
Tuberculosis exposure, infection and disease in children: a systematic diagnostic approach
Abstract
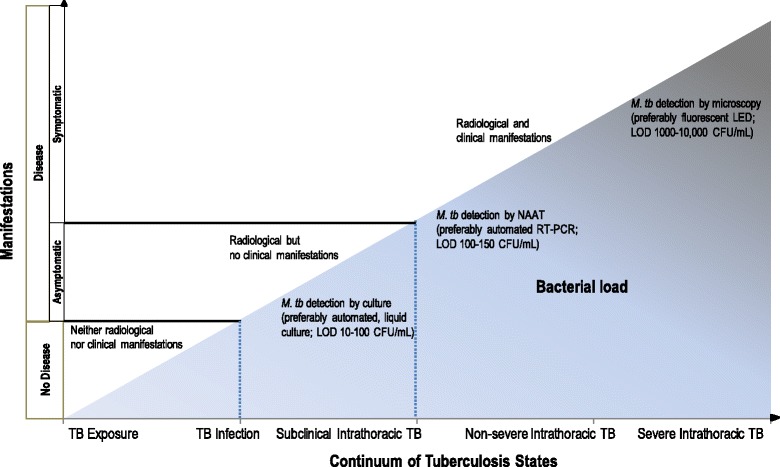
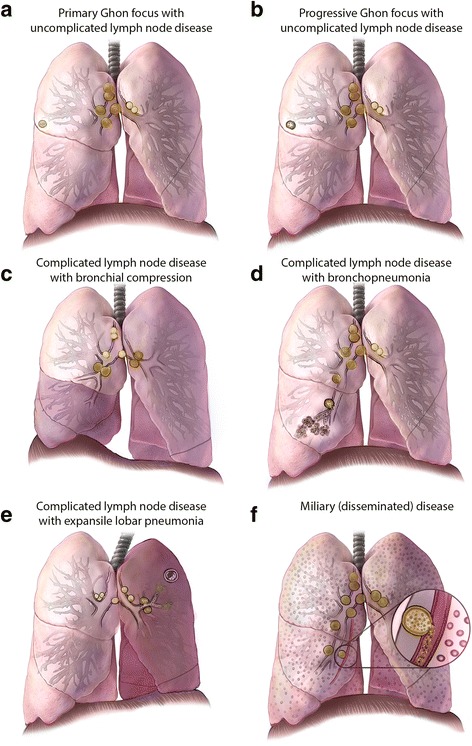
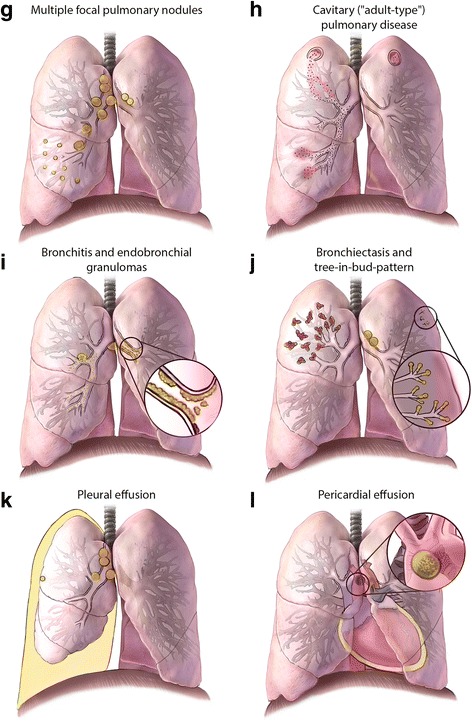
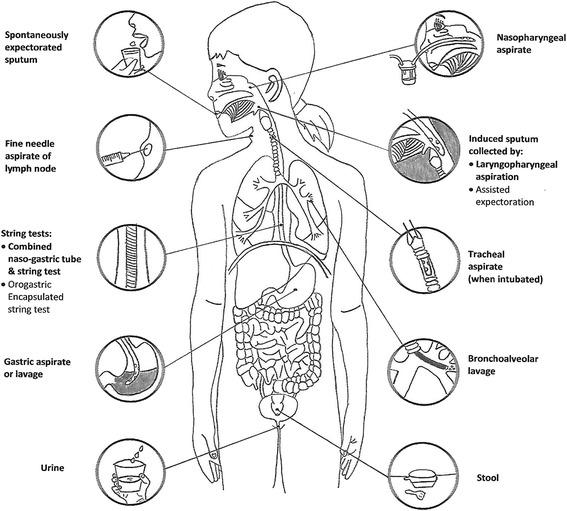
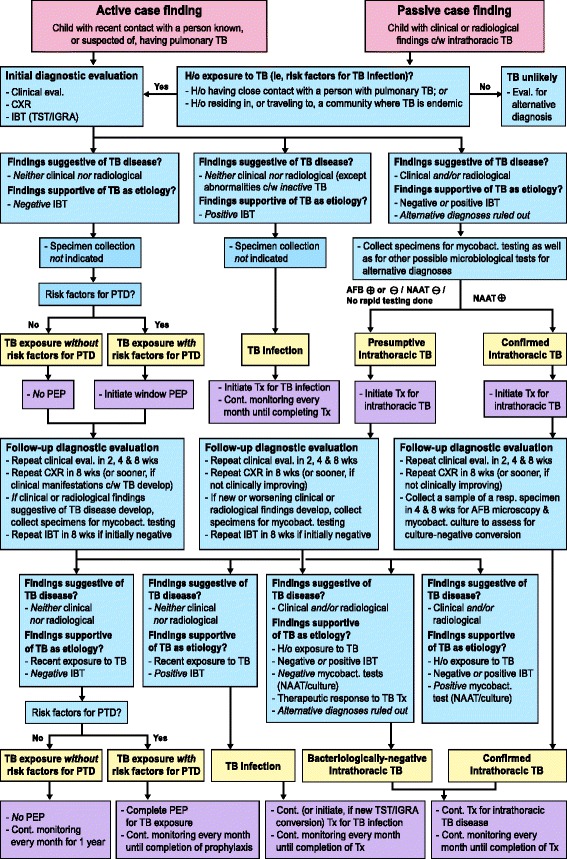
The accurate diagnosis of tuberculosis (TB) in children remains challenging. A myriad of common childhood diseases can present with similar symptoms and signs, and differentiating between exposure and infection, as well as infection and disease can be problematic. The paucibacillary nature of childhood TB complicates bacteriological confirmation and specimen collection is difficult. In most instances intrathoracic TB remains a clinical diagnosis. TB infection and disease represent a dynamic continuum from TB exposure with/without infection, to subclinical/incipient disease, to non-severe and severe disease. The clinical spectrum of intrathoracic TB in children is broad, and the classification of clinical, radiological, endoscopic, and laboratory findings into recognized clinical syndromes allows a more refined diagnostic approach in order to minimize both under- and over-diagnosis. Bacteriological confirmation can be improved significantly by collecting multiple, high-quality specimens from the most appropriate source. Mycobacterial testing should include traditional smear microscopy and culture, as well as nucleic acid amplification testing. A systematic approach to the child with recent exposure to TB, or with clinical and radiological findings compatible with this diagnosis, should allow pragmatic classification as TB exposure, infection, or disease to facilitate timely and appropriate management. It is important to also assess risk factors for TB disease progression and to undertake follow-up evaluations to monitor treatment response and ongoing evidence supporting a TB, or alternative, diagnosis.
Keywords: Algorithm; Diagnostic techniques and procedures; Latent tuberculosis; Risk factors; Specimen handling.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
