

Evaluating the impact of varied compliance to lung cancer screening recommendations using a microsimulation model
- PMID: 28702814
- PMCID: PMC5880208
- DOI: 10.1007/s10552-017-0907-x
Evaluating the impact of varied compliance to lung cancer screening recommendations using a microsimulation model
Abstract
Background: The US preventive services task force (USPSTF) recently recommended that individuals aged 55-80 with heavy smoking history be annually screened by low-dose computed tomography (LDCT), thereby extending the stopping age from 74 to 80 compared to the national lung screening trial (NLST) entry criterion. This decision was made partly with model-based analyses from cancer intervention and surveillance modeling network (CISNET), which assumed perfect compliance to screening.
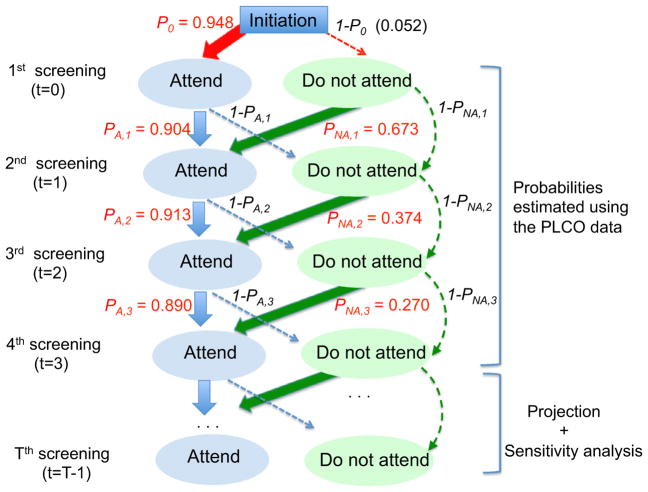
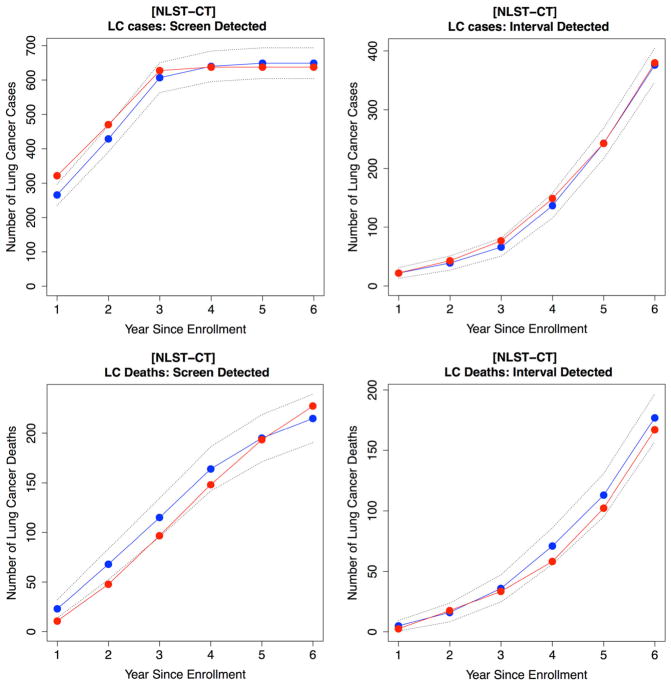
Methods: As part of CISNET, we developed a microsimulation model for lung cancer (LC) screening and calibrated and validated it using data from NLST and the prostate, lung, colorectal, and ovarian cancer screening trial (PLCO), respectively. We evaluated population-level outcomes of the lifetime screening program recommended by the USPSTF by varying screening compliance levels.
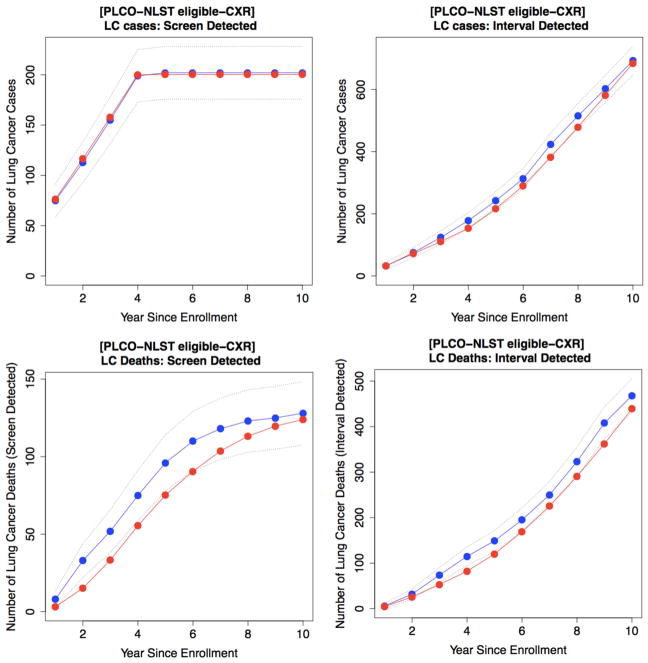
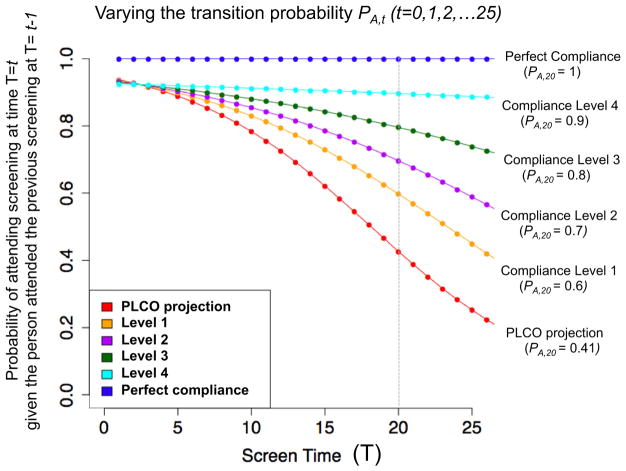
Results: Validation using PLCO shows that our model reproduces observed PLCO outcomes, predicting 884 LC cases [Expected(E)/Observed(O) = 0.99; CI 0.92-1.06] and 563 LC deaths (E/O = 0.94 CI 0.87-1.03) in the screening arm that has an average compliance rate of 87.9% over four annual screening rounds. We predict that perfect compliance to the USPSTF recommendation saves 501 LC deaths per 100,000 persons in the 1950 U.S. birth cohort; however, assuming that compliance behaviors extrapolated and varied from PLCO reduces the number of LC deaths avoided to 258, 230, and 175 as the average compliance rate over 26 annual screening rounds changes from 100 to 46, 39, and 29%, respectively.
Conclusion: The implementation of the USPSTF recommendation is expected to contribute to a reduction in LC deaths, but the magnitude of the reduction will likely be heavily influenced by screening compliance.
Keywords: CISNET; CT screening; Lung cancer; Microsimulation; NLST; Public health policy; USPSTF.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
