

Timed Delivery of Therapy Enhances Functional Muscle Regeneration
- PMID: 28703489
- PMCID: PMC5641972
- DOI: 10.1002/adhm.201700202
Timed Delivery of Therapy Enhances Functional Muscle Regeneration
Abstract
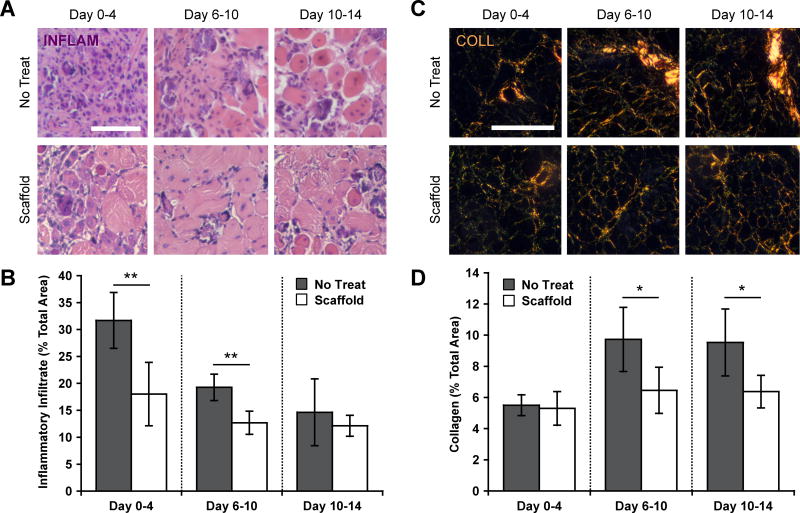
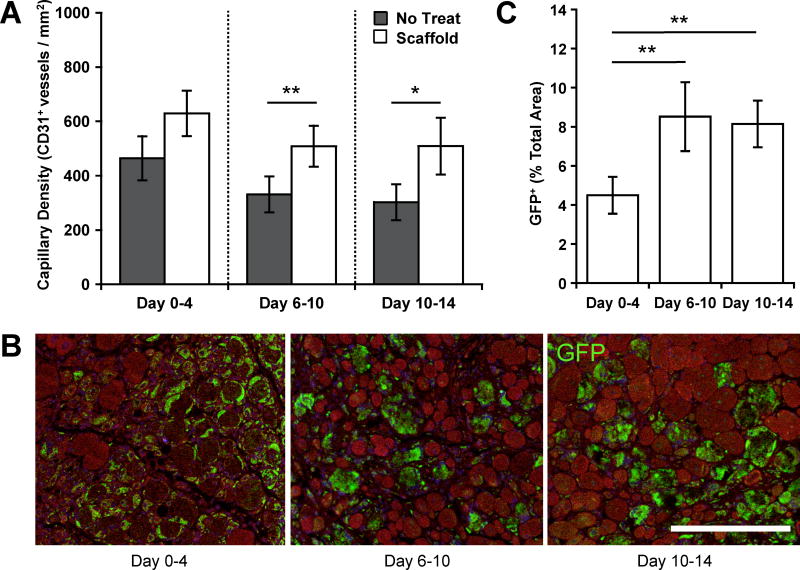
Cell transplantation is a promising therapeutic strategy for the treatment of traumatic muscle injury in humans. Previous investigations have typically focused on the identification of potent cell and growth factor treatments and optimization of spatial control over delivery. However, the optimal time point for cell transplantation remains unclear. Here, this study reports how myoblast and morphogen delivery timed to coincide with specific phases of the inflammatory response affects donor cell engraftment and the functional repair of severely injured muscle. Delivery of a biomaterial-based therapy timed with the peak of injury-induced inflammation leads to potent early and long-term regenerative benefits. Diminished inflammation and fibrosis, enhanced angiogenesis, and increased cell engraftment are seen during the acute stage following optimally timed treatment. Over the long term, treatment during peak inflammation leads to enhanced functional regeneration, as indicated by reduced chronic inflammation and fibrosis along with increased tissue perfusion and muscle contractile force. Treatments initiated immediately after injury or after inflammation had largely resolved provided more limited benefits. These results demonstrate the importance of appropriately timing the delivery of biologic therapy in the context of muscle regeneration. Biomaterial-based timed delivery can likely be applied to other tissues and is of potential wide utility in regenerative medicine.
Keywords: cell therapy; controlled delivery; ferrogel scaffolds; inflammation kinetics; magnetic biomaterials.
© 2017 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim.
Figures


References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
