

Fistulizing Crohn's Disease
- PMID: 28703786
- PMCID: PMC5539341
- DOI: 10.1038/ctg.2017.33
Fistulizing Crohn's Disease
Abstract
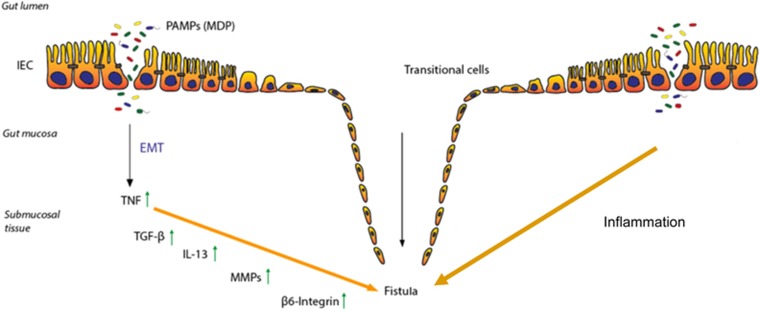
Fistulas still represent one of the most important complications in patients with Crohn's disease (CD). At least one third of CD patients suffer from fistulas during their disease course and amongst them longstanding remission of complex fistulas occurs only in about one third. So far, fistula pathogenesis is only partially understood. From a histopathological view, a fistula is a tube covered by flat epithelial cells. Current research suggests that the driving force for fistula development is epithelial-to-mesenchymal transition (EMT). Around the fistula, high levels of tumor necrosis factor (TNF), IL-13, and TGFβ can be detected and recent studies indicated an involvement of the intestinal microbiota. Fistula diagnosis requires clinical and surgical assessment, radiologic investigations, e.g., magnet resonance imaging and endoscopy. Routine medical treatment of fistulas includes antibiotics, immunosuppressives, and anti-TNF antibodies. There is no well-established role for calcineurin inhibitors in fistula treatment, corticosteroids appear to be even contra-productive. A promising novel approach might be the application of adipose tissue-derived or bone marrow-derived mesenchymal stem cells that have been studied recently. Due to insufficient efficacy of medical treatment and recurrence of fistulas, surgical interventions are frequently necessary. Further research is needed to better understand fistula pathogenesis aiming to develop novel treatment option for our patients.
Conflict of interest statement
Figures
Similar articles
-
[Perianal fistulas in CED: from mouse model to clinic].Ther Umsch. 2019 Jan;75(5):287-294. doi: 10.1024/0040-5930/a001000. Ther Umsch. 2019. PMID: 30700244 Review. German.
-
[Effectiveness of anti-TNF alpha antibodies in treatment of fistulizing Crohn's disease].Przegl Lek. 2011;68(9):602-5. Przegl Lek. 2011. PMID: 22335009 Polish.
-
Eribulin Does Not Prevent Epithelial-to-Mesenchymal Transition in HT-29 Intestinal Epithelial Cells.Inflamm Intest Dis. 2018 Jul;2(4):211-218. doi: 10.1159/000490052. Epub 2018 Jul 10. Inflamm Intest Dis. 2018. PMID: 30221148 Free PMC article.
-
Treatment of perianal fistulas in Crohn's disease by local injection of antibody to TNF-alpha accounts for a favourable clinical response in selected cases: a pilot study.Scand J Gastroenterol. 2006 Sep;41(9):1064-72. doi: 10.1080/00365520600609941. Scand J Gastroenterol. 2006. PMID: 16938720
-
Fistula treatment: The unresolved challenge.Dig Dis. 2010;28(3):556-64. doi: 10.1159/000320416. Epub 2010 Sep 30. Dig Dis. 2010. PMID: 20926886 Review.
Cited by
-
MMP9 expression in intestinal fistula from patients with fistulizing CD and from human xenograft mouse model.Tissue Barriers. 2022 Apr 3;10(2):1994350. doi: 10.1080/21688370.2021.1994350. Epub 2021 Oct 28. Tissue Barriers. 2022. PMID: 34709129 Free PMC article.
-
Gastrocolic fistula in Crohn's disease detected by oral agent contrast-enhanced ultrasound: A case report of a novel ultrasound modality.World J Gastroenterol. 2020 May 7;26(17):2119-2125. doi: 10.3748/wjg.v26.i17.2119. World J Gastroenterol. 2020. PMID: 32536779 Free PMC article.
-
Prolonged Time to Diagnosis of Crohn's Disease in Patients With Perianal Fistulas Negatively Affects Long-Term Outcomes.J Crohns Colitis. 2025 Mar 5;19(3):jjae146. doi: 10.1093/ecco-jcc/jjae146. J Crohns Colitis. 2025. PMID: 39297524 Free PMC article.
-
Current concepts in the pathogenesis of cryptoglandular perianal fistula.J Int Med Res. 2021 Feb;49(2):300060520986669. doi: 10.1177/0300060520986669. J Int Med Res. 2021. PMID: 33595349 Free PMC article. Review.
-
Enterocutaneous Fistula in a Patient with Crohn's Disease After Internalization of a Foreign Body into the Gastrointestinal Tract.J Clin Med. 2025 Mar 28;14(7):2327. doi: 10.3390/jcm14072327. J Clin Med. 2025. PMID: 40217777 Free PMC article.
References
-
- Schwartz DA et al. The natural history of fistulizing Crohn's disease in Olmsted County, Minnesota. Gastroenterology 2002; 122: 875–880. - PubMed
-
- Peyrin-Biroulet L et al. The natural history of adult Crohn's disease in population-based cohorts. Am J Gastroenterol 2010; 105: 289–297. - PubMed
-
- Cosnes J et al. Long-term evolution of disease behavior of Crohn's disease. Inflamm Bowel Dis 2002; 8: 244–250. - PubMed
-
- Gower-Rousseau C et al. Epidemiology of inflammatory bowel diseases: new insights from a French population-based registry (EPIMAD). Dig Liver Dis 2013; 45: 89–94. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
