

Measles Outbreak - Minnesota April-May 2017
- PMID: 28704350
- PMCID: PMC5687591
- DOI: 10.15585/mmwr.mm6627a1
Measles Outbreak - Minnesota April-May 2017
Abstract
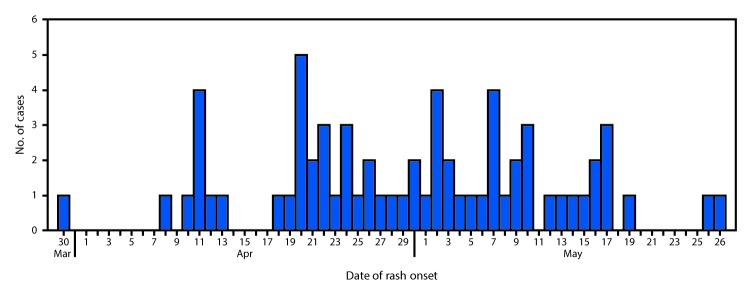
On April 10, 2017, the Minnesota Department of Health (MDH) was notified about a suspected measles case. The patient was a hospitalized child aged 25 months who was evaluated for fever and rash, with onset on April 8. The child had no history of receipt of measles-mumps-rubella (MMR) vaccine and no travel history or known exposure to measles. On April 11, MDH received a report of a second hospitalized, unvaccinated child, aged 34 months, with an acute febrile rash illness with onset on April 10. The second patient's sibling, aged 19 months, who had also not received MMR vaccine, had similar symptoms, with rash onset on March 30. Real-time reverse transcription-polymerase chain reaction (rRT-PCR) testing of nasopharyngeal swab or throat specimens performed at MDH confirmed measles in the first two patients on April 11, and in the third patient on April 13; subsequent genotyping identified genotype B3 virus in all three patients, who attended the same child care center. MDH instituted outbreak investigation and response activities in collaboration with local health departments, health care facilities, child care facilities, and schools in affected settings. Because the outbreak occurred in a community with low MMR vaccination coverage, measles spread rapidly, resulting in thousands of exposures in child care centers, schools, and health care facilities. By May 31, 2017, a total of 65 confirmed measles cases had been reported to MDH (Figure 1); transmission is ongoing.
Conflict of interest statement
Figures
References
-
- Council of State and Territorial Epidemiologists. Public health reporting and national notification for measles. Atlanta, GA: Council of State and Territorial Epidemiologists; 2012. http://c.ymcdn.com/sites/www.cste.org/resource/resmgr/ps/12-id-07final.pdf
-
- McLean HQ, Fiebelkorn AP, Temte JL, Wallace GS. Prevention of measles, rubella, congenital rubella syndrome, and mumps, 2013: summary recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 2013;62(No. RR-4). - PubMed
-
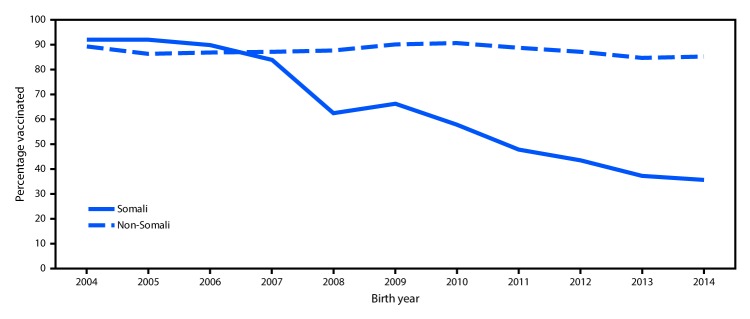
- Bahta L, Ashkir A. Addressing MMR vaccine resistance in Minnesota’s Somali community. Minn Med 2015;98:33–6. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
