

Influence of lung CT changes in chronic obstructive pulmonary disease (COPD) on the human lung microbiome
- PMID: 28704452
- PMCID: PMC5509234
- DOI: 10.1371/journal.pone.0180859
Influence of lung CT changes in chronic obstructive pulmonary disease (COPD) on the human lung microbiome
Abstract
Background: Changes in microbial community composition in the lung of patients suffering from moderate to severe COPD have been well documented. However, knowledge about specific microbiome structures in the human lung associated with CT defined abnormalities is limited.
Methods: Bacterial community composition derived from brush samples from lungs of 16 patients suffering from different CT defined subtypes of COPD and 9 healthy subjects was analyzed using a cultivation independent barcoding approach applying 454-pyrosequencing of 16S rRNA gene fragment amplicons.
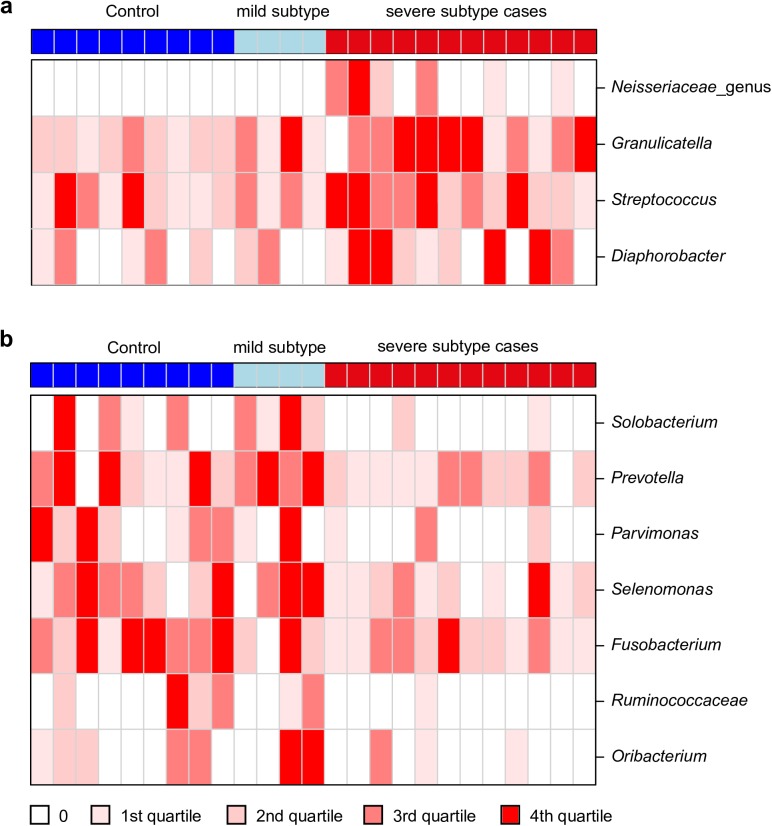
Results: We could show that bacterial community composition in patients with changes in CT (either airway or emphysema type changes, designated as severe subtypes) was different from community composition in lungs of patients without visible changes in CT as well as from healthy subjects (designated as mild COPD subtype and control group) (PC1, Padj = 0.002). Higher abundance of Prevotella in samples from patients with mild COPD subtype and from controls and of Streptococcus in the severe subtype cases mainly contributed to the separation of bacterial communities of subjects. No significant effects of treatment with inhaled glucocorticoids on bacterial community composition were detected within COPD cases with and without abnormalities in CT in PCoA. Co-occurrence analysis suggests the presence of networks of co-occurring bacteria. Four communities of positively correlated bacteria were revealed. The microbial communities can clearly be distinguished by their associations with the CT defined disease phenotype.
Conclusion: Our findings indicate that CT detectable structural changes in the lung of COPD patients, which we termed severe subtypes, are associated with alterations in bacterial communities, which may induce further changes in the interaction between microbes and host cells. This might result in a changed interplay with the host immune system.
Conflict of interest statement
Figures



Similar articles
-
Lung microbiome composition and bronchial epithelial gene expression in patients with COPD versus healthy individuals: a bacterial 16S rRNA gene sequencing and host transcriptomic analysis.Lancet Microbe. 2021 Jul;2(7):e300-e310. doi: 10.1016/S2666-5247(21)00035-5. Epub 2021 Apr 23. Lancet Microbe. 2021. PMID: 35544166
-
The lung tissue microbiota of mild and moderate chronic obstructive pulmonary disease.Microbiome. 2018 Jan 9;6(1):7. doi: 10.1186/s40168-017-0381-4. Microbiome. 2018. PMID: 29316977 Free PMC article.
-
Metagenome and Metatranscriptome Profiling of Moderate and Severe COPD Sputum in Taiwanese Han Males.PLoS One. 2016 Jul 18;11(7):e0159066. doi: 10.1371/journal.pone.0159066. eCollection 2016. PLoS One. 2016. PMID: 27428540 Free PMC article.
-
The lung microbiome dynamics between stability and exacerbation in chronic obstructive pulmonary disease (COPD): Current perspectives.Respir Med. 2019 Oct;157:1-6. doi: 10.1016/j.rmed.2019.08.012. Epub 2019 Aug 21. Respir Med. 2019. PMID: 31450162 Review.
-
The composition of lung microbiome in lung cancer: a systematic review and meta-analysis.BMC Microbiol. 2021 Nov 11;21(1):315. doi: 10.1186/s12866-021-02375-z. BMC Microbiol. 2021. PMID: 34763672 Free PMC article.
Cited by
-
Exploring the Role of Gut-Lung Interactions in COPD Pathogenesis: A Comprehensive Review on Microbiota Characteristics and Inflammation Modulation.Chronic Obstr Pulm Dis. 2024 May 29;11(3):311-325. doi: 10.15326/jcopdf.2023.0442. Chronic Obstr Pulm Dis. 2024. PMID: 38563747 Free PMC article.
-
Respiratory microbiota and radiomics features in the stable COPD patients.Respir Res. 2023 May 12;24(1):131. doi: 10.1186/s12931-023-02434-1. Respir Res. 2023. PMID: 37173744 Free PMC article.
-
Microbiota and Tuberculosis: A Potential Role of Probiotics, and Postbiotics.Front Nutr. 2021 May 7;8:626254. doi: 10.3389/fnut.2021.626254. eCollection 2021. Front Nutr. 2021. PMID: 34026804 Free PMC article. Review.
-
Chronic obstructive pulmonary disease upper airway microbiota alpha diversity is associated with exacerbation phenotype: a case-control observational study.Respir Res. 2019 Jun 7;20(1):114. doi: 10.1186/s12931-019-1080-4. Respir Res. 2019. PMID: 31174538 Free PMC article.
-
Airway microbiome-immune crosstalk in chronic obstructive pulmonary disease.Front Immunol. 2023 Jan 17;13:1085551. doi: 10.3389/fimmu.2022.1085551. eCollection 2022. Front Immunol. 2023. PMID: 36741369 Free PMC article. Review.
References
-
- WHO. Chronic obstructive pulmonary disease (COPD). http://wwwwhoint/mediacentre/factsheets/fs315/en/. 2015;(Fact sheet N°315, updated January 2015).
-
- Vogelmeier CF, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ, Bourbeau J, et al. Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Lung Disease 2017 Report. Respirology. 2017;22(3):575–601. doi: 10.1111/resp.13012 - DOI - PubMed
-
- Singh D, Roche N, Halpin D, Agusti A, Wedzicha JA, Martinez FJ. Current Controversies in the Pharmacological Treatment of Chronic Obstructive Pulmonary Disease. American Journal of Respiratory and Critical Care Medicine. 2016;194(5):541–9. doi: 10.1164/rccm.201606-1179PP - DOI - PubMed
-
- Ziegler-Heitbrock L, Frankenberger M, Heimbeck I, Burggraf D, Wjst M, Häussinger K, et al. The EvA study: aims and strategy. European Respiratory Journal. 2012;40(4):823–9. doi: 10.1183/09031936.00142811 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
