

The prognostic value of lymph node yield in the earliest stage of colorectal cancer: a multicenter cohort study
- PMID: 28705200
- PMCID: PMC5512847
- DOI: 10.1186/s12916-017-0892-7
The prognostic value of lymph node yield in the earliest stage of colorectal cancer: a multicenter cohort study
Abstract
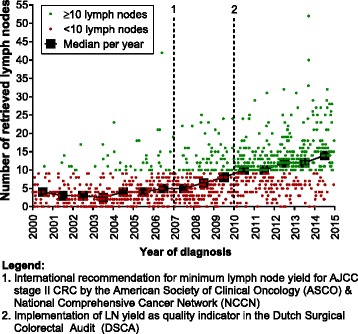
Background: In patients with stage II colorectal cancer (CRC) the number of surgically retrieved lymph nodes (LNs) is associated with prognosis, resulting in a minimum of 10-12 retrieved LNs being recommended for this stage. Current guidelines do not provide a recommendation regarding LN yield in T1 CRC. Studies evaluating LN yield in T1 CRC suggest that such high LN yields are not feasible in this early stage, and a lower LN yield might be appropriate. We aimed to validate the cut-off of 10 retrieved LNs on risk for recurrent cancer and detection of LN metastasis (LNM) in T1 CRC, and explored whether this number is feasible in clinical practice.
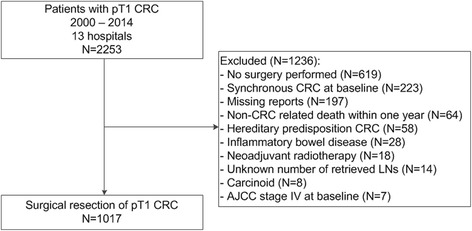
Methods: Patients diagnosed with T1 CRC and treated with surgical resection between 2000 and 2014 in thirteen participating hospitals were selected from the Netherlands Cancer Registry. Medical records were reviewed to collect additional information. The association between LN yield and recurrence and LNM respectively were analyzed using 10 LNs as cut-off. Propensity score analysis using inverse probability weighting (IPW) was performed to adjust for clinical and histological confounding factors (i.e., age, sex, tumor location, size and morphology, presence of LNM, lymphovascular invasion, depth of submucosal invasion, and grade of differentiation).
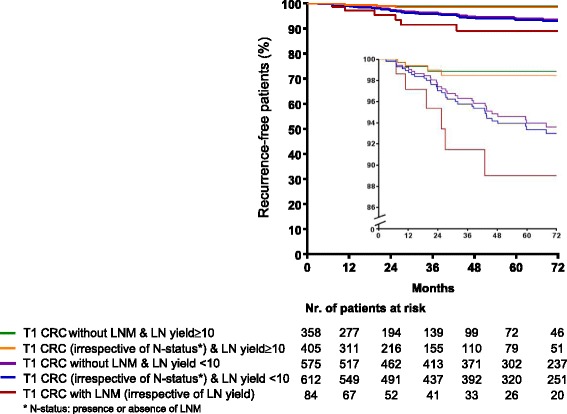
Results: In total, 1017 patients with a median follow-up time of 49.0 months (IQR 19.6-81.5) were included. Four-hundred five patients (39.8%) had a LN yield ≥ 10. Forty-one patients (4.0%) developed recurrence. LN yield ≥ 10 was independently associated with a decreased risk for recurrence (IPW-adjusted HR 0.20; 95% CI 0.06-0.67; P = 0.009). LNM were detected in 84 patients (8.3%). LN yield ≥ 10 was independently associated with increased detection of LNM (IPW-adjusted OR 2.27; 95% CI 1.39-3.69; P = 0.001).
Conclusions: In this retrospective observational study, retrieving < 10 LNs was associated with an increased risk of CRC recurrence, advocating the importance to perform an appropriate oncologic resection of the draining LNs and diligent LN search when patients with T1 CRC at high-risk for LNM are referred for surgical resection. Given that both gastroenterologists, surgeons and pathologists will encounter T1 CRCs with increasing frequency due to the introduction of national screening programs, awareness on the consequences of an inadequate LN retrieval is of utmost importance.
Keywords: Lymph node metastasis; Lymph node retrieval; Malignant polyps; T1 colorectal carcinoma.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
