

Palliative Care in Heart Failure: The PAL-HF Randomized, Controlled Clinical Trial
- PMID: 28705314
- PMCID: PMC5664956
- DOI: 10.1016/j.jacc.2017.05.030
Palliative Care in Heart Failure: The PAL-HF Randomized, Controlled Clinical Trial
Abstract
Background: Advanced heart failure (HF) is characterized by high morbidity and mortality. Conventional therapy may not sufficiently reduce patient suffering and maximize quality of life.
Objectives: The authors investigated whether an interdisciplinary palliative care intervention in addition to evidence-based HF care improves certain outcomes.
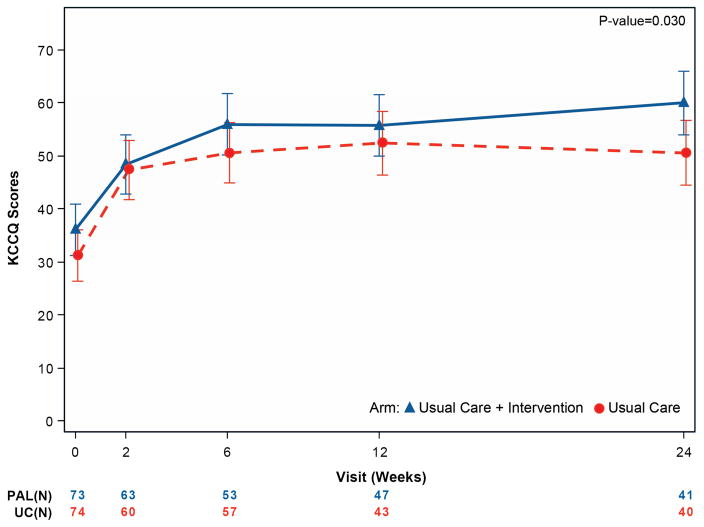
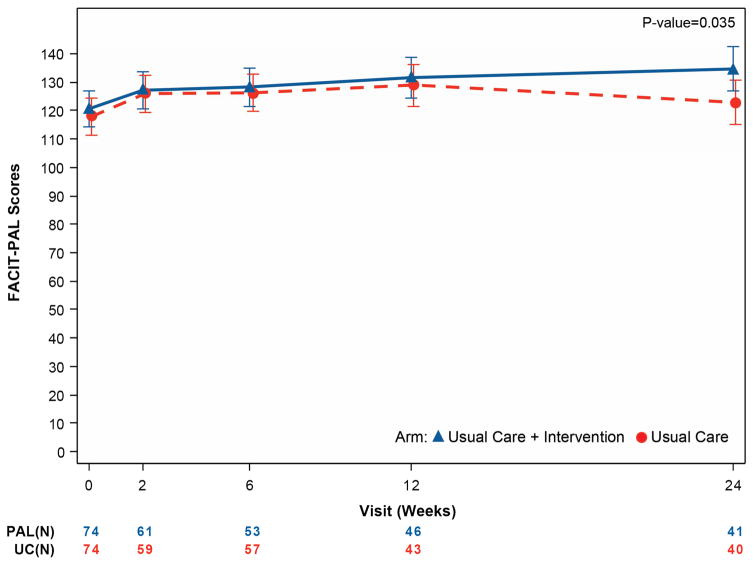
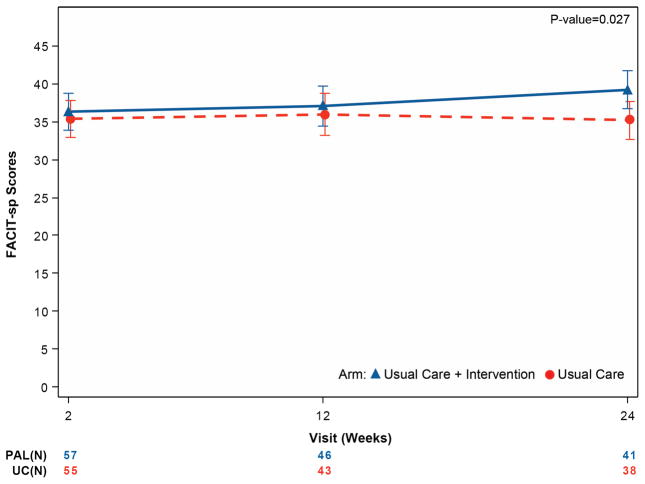
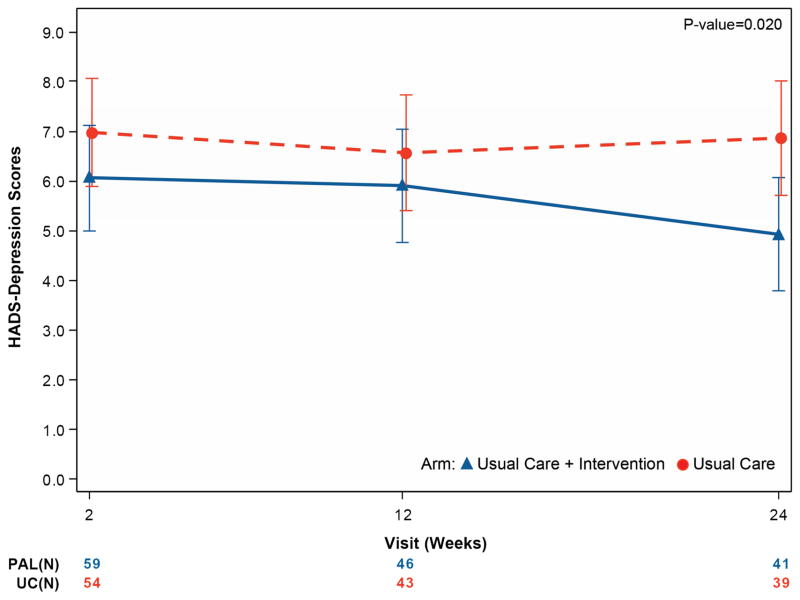
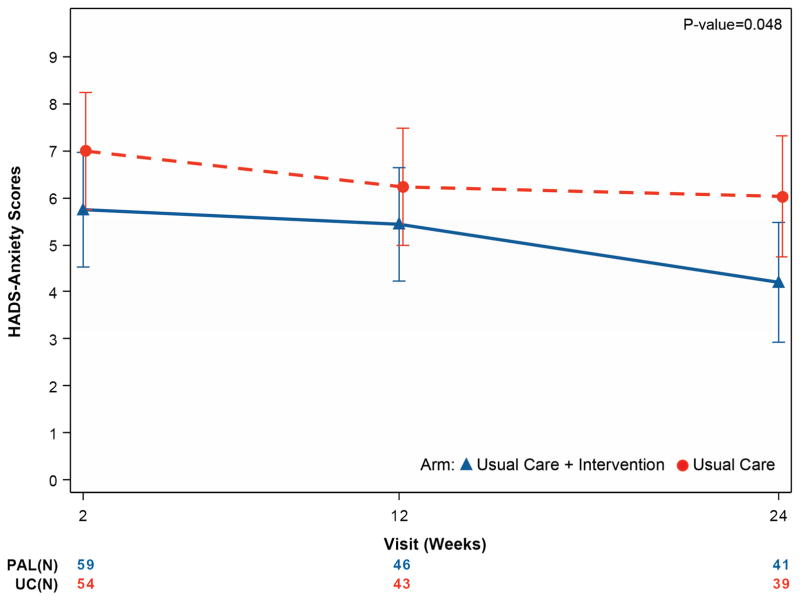
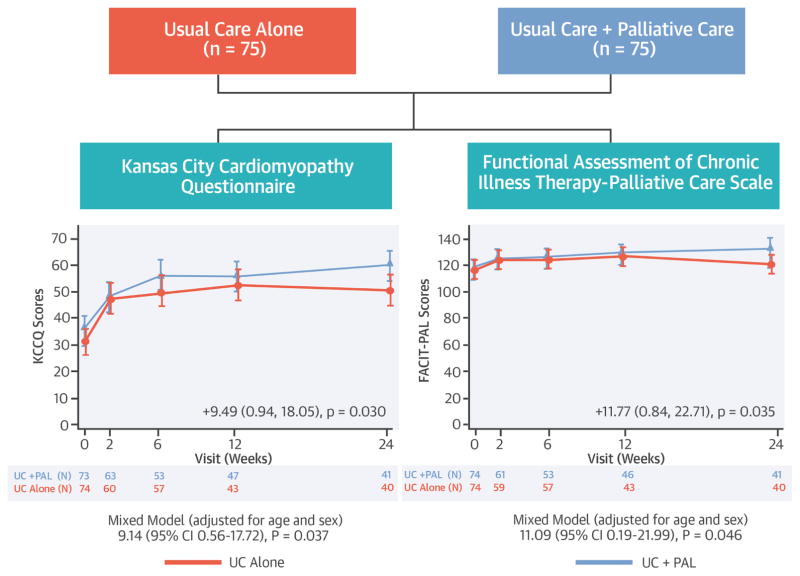
Methods: The authors randomized 150 patients with advanced HF between August 15, 2012, and June 25, 2015, to usual care (UC) (n = 75) or UC plus a palliative care intervention (UC + PAL) (n = 75) at a single center. Primary endpoints were 2 quality-of-life measurements, the Kansas City Cardiomyopathy Questionnaire (KCCQ) overall summary and the Functional Assessment of Chronic Illness Therapy-Palliative Care scale (FACIT-Pal), assessed at 6 months. Secondary endpoints included assessments of depression and anxiety (measured via the Hospital Anxiety and Depression Scale [HADS]), spiritual well-being (measured via the FACIT-Spiritual Well-Being scale [FACIT-Sp]), hospitalizations, and mortality.
Results: Patients randomized to UC + PAL versus UC alone had clinically significant incremental improvement in KCCQ and FACIT-Pal scores from randomization to 6 months (KCCQ difference = 9.49 points, 95% confidence interval [CI]: 0.94 to 18.05, p = 0.030; FACIT-Pal difference = 11.77 points, 95% CI: 0.84 to 22.71, p = 0.035). Depression improved in UC + PAL patients (HADS-depression difference = -1.94 points; p = 0.020) versus UC-alone patients, with similar findings for anxiety (HADS-anxiety difference = -1.83 points; p = 0.048). Spiritual well-being was improved in UC + PAL versus UC-alone patients (FACIT-Sp difference = 3.98 points; p = 0.027). Randomization to UC + PAL did not affect rehospitalization or mortality.
Conclusions: An interdisciplinary palliative care intervention in advanced HF patients showed consistently greater benefits in quality of life, anxiety, depression, and spiritual well-being compared with UC alone. (Palliative Care in Heart Failure [PAL-HF]; NCT01589601).
Keywords: heart failure; palliative care; quality of life.
Copyright © 2017 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Mending the Soul When the Heart Is Broken.J Am Coll Cardiol. 2017 Jul 18;70(3):342-343. doi: 10.1016/j.jacc.2017.05.058. J Am Coll Cardiol. 2017. PMID: 28705315 No abstract available.
References
-
- Yancy CW, Jessup M, Bozkurt B, et al. 2016 ACC/AHA/HFSA focused update on new pharmacological therapy for heart failure: an update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol. 2016 May 17; pii: S0735-1097(16)33024-8.
-
- Go AS, Mozaffarian D, Roger VL, et al. Executive summary: heart disease and stroke statistics--2013 update: a report from the American Heart Association. Circulation. 2013;127:143–52. - PubMed
-
- Selman L, Beynon T, Higginson IJ, Harding R. Psychological, social and spiritual distress at the end of life in heart failure patients. Curr Opin Support Palliat Care. 2007;1:260–6. - PubMed
-
- Bekelman DB, Havranek EP, Becker DM, et al. Symptoms, depression, and quality of life in patients with heart failure. J Card Fail. 2007;13:643–8. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
