

Electrical and Structural Substrate of Arrhythmogenic Right Ventricular Cardiomyopathy Determined Using Noninvasive Electrocardiographic Imaging and Late Gadolinium Magnetic Resonance Imaging
- PMID: 28705875
- PMCID: PMC5533087
- DOI: 10.1161/CIRCEP.116.005105
Electrical and Structural Substrate of Arrhythmogenic Right Ventricular Cardiomyopathy Determined Using Noninvasive Electrocardiographic Imaging and Late Gadolinium Magnetic Resonance Imaging
Abstract
Background: Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a significant cause of sudden cardiac death in the young. Improved noninvasive assessment of ARVC and better understanding of the disease substrate are important for improving patient outcomes.
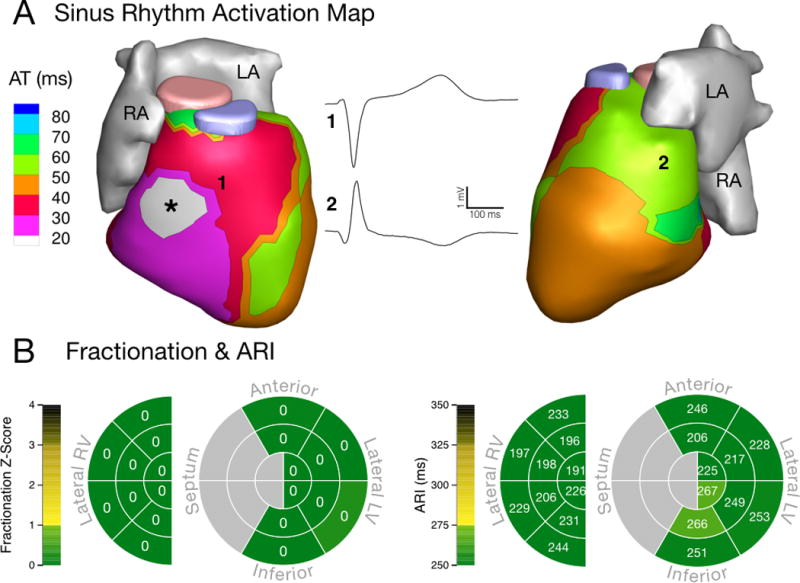
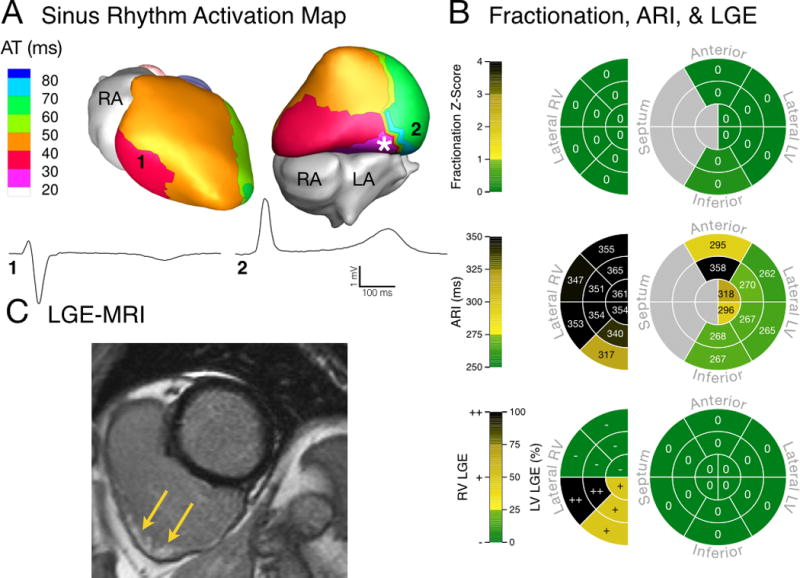
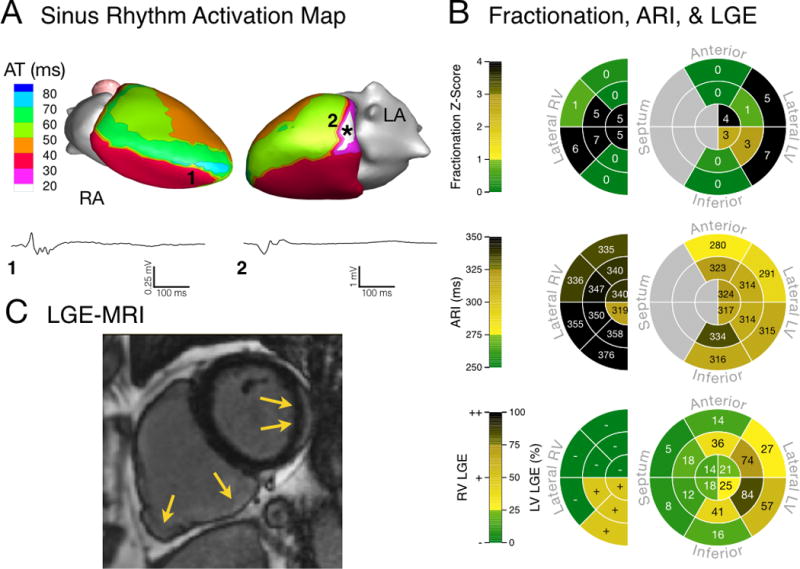
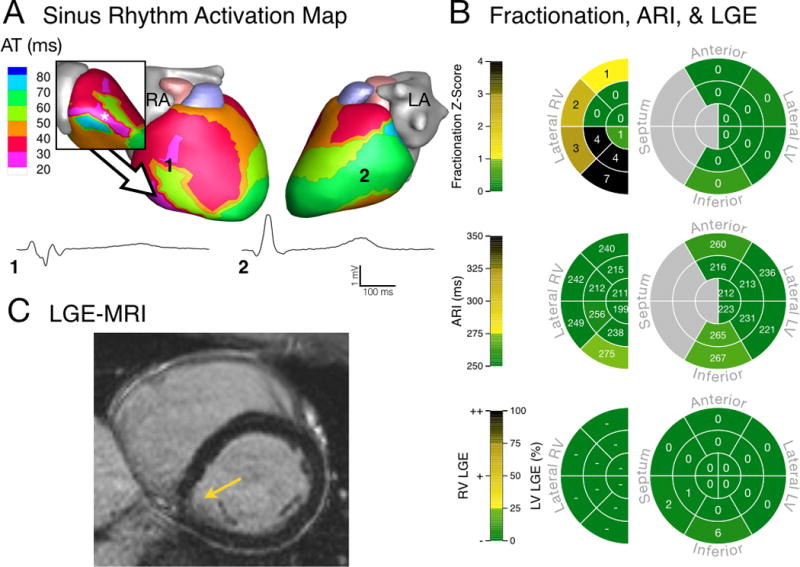
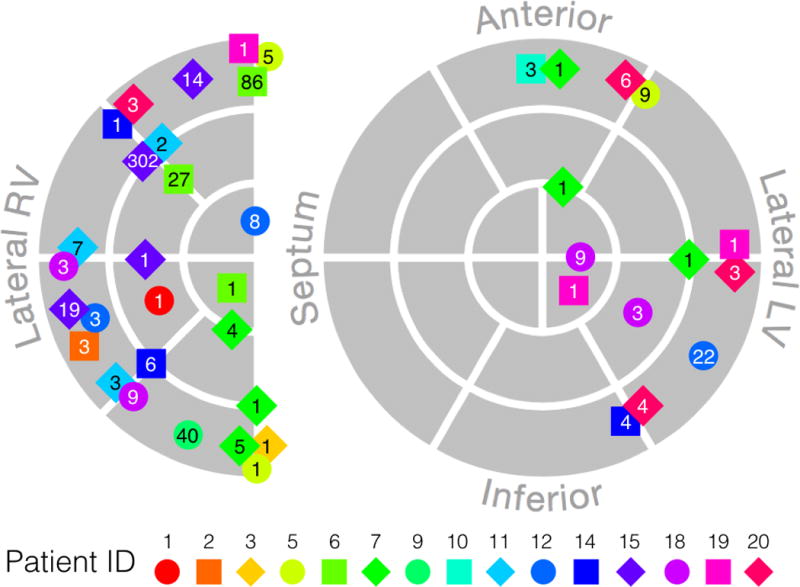
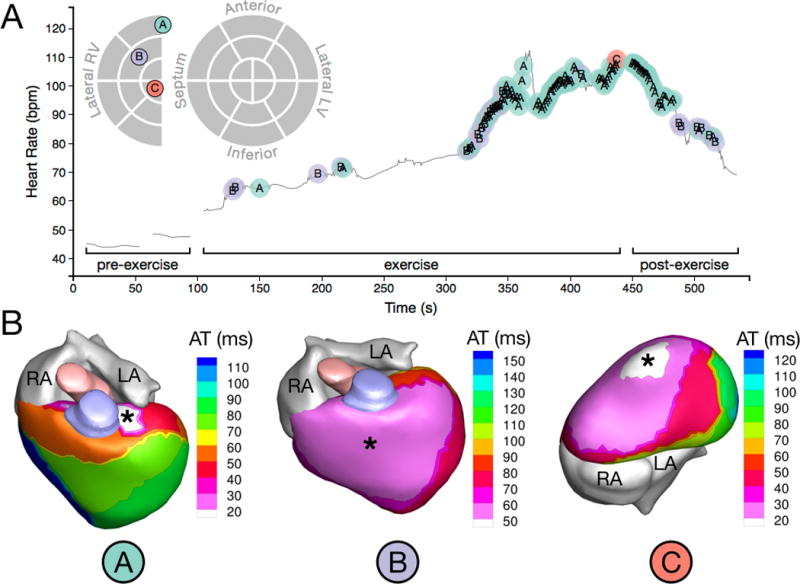
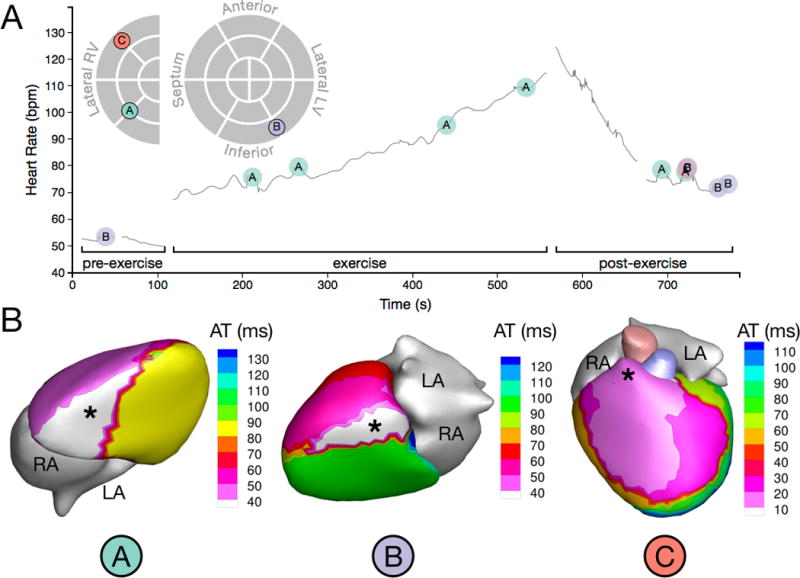
Methods and results: We studied 20 genotyped ARVC patients with a broad spectrum of disease using electrocardiographic imaging (a method for noninvasive cardiac electrophysiology mapping) and advanced late gadolinium enhancement cardiac magnetic resonance scar imaging. Compared with 20 healthy controls, ARVC patients had longer ventricular activation duration (median, 52 versus 42 ms; P=0.007) and prolonged mean epicardial activation-recovery intervals (a surrogate for local action potential duration; median, 275 versus 241 ms; P=0.014). In these patients, we observed abnormal and varied epicardial activation breakthrough locations and regions of nonuniform conduction and fractionated electrograms. Nonuniform conduction and fractionated electrograms were present in the early concealed phase of ARVC. Electrophysiological abnormalities colocalized with late gadolinium enhancement scar, indicating a relationship with structural disease. Premature ventricular contractions were common in ARVC patients with variable initiation sites in both ventricles. Premature ventricular contraction rate increased with exercise, and within anatomic segments, it correlated with prolonged repolarization, electric markers of scar, and late gadolinium enhancement (all P<0.001).
Conclusions: Electrocardiographic imaging reveals electrophysiological substrate properties that differ in ARVC patients compared with healthy controls. A novel mechanistic finding is the presence of repolarization abnormalities in regions where ventricular ectopy originates. The results suggest a potential role for electrocardiographic imaging and late gadolinium enhancement in early diagnosis and noninvasive follow-up of ARVC patients.
Keywords: arrhythmogenic right ventricular dysplasia; cardiac electrophysiology; early diagnosis; gadolinium; heart ventricles.
© 2017 American Heart Association, Inc.
Figures
Comment in
-
Mapping the Electrical Substrate in Arrhythmogenic Right Ventricular Cardiomyopathy: There Is More Than Meets the Eye.Circ Arrhythm Electrophysiol. 2017 Jul;10(7):e005524. doi: 10.1161/CIRCEP.117.005524. Circ Arrhythm Electrophysiol. 2017. PMID: 28705880 No abstract available.
-
Letter by Di Marco et al Regarding Article, "Electrical and Structural Substrate of Arrhythmogenic Right Ventricular Cardiomyopathy Determined Using Noninvasive Electrocardiographic Imaging and Late Gadolinium Magnetic Resonance Imaging".Circ Arrhythm Electrophysiol. 2017 Oct;10(10):e005687. doi: 10.1161/CIRCEP.117.005687. Circ Arrhythm Electrophysiol. 2017. PMID: 29038105 No abstract available.
-
Response by Andrews et al to Letter Regarding Article, "Electrical and Structural Substrate of Arrhythmogenic Right Ventricular Cardiomyopathy Determined Using Noninvasive Electrocardiographic Imaging and Late Gadolinium Magnetic Resonance Imaging".Circ Arrhythm Electrophysiol. 2017 Oct;10(10):e005768. doi: 10.1161/CIRCEP.117.005768. Circ Arrhythm Electrophysiol. 2017. PMID: 29038106 Free PMC article. No abstract available.
References
-
- Sen-Chowdhry S, Morgan RD, Chambers JC, McKenna WJ. Arrhythmogenic cardiomyopathy: etiology, diagnosis, and treatment. Annu Rev Med. 2010;61:233–253. - PubMed
-
- Marcus FI, McKenna WJ, Sherrill D, Basso C, Bauce B, Bluemke DA, Calkins H, Corrado D, Cox MGPJ, Daubert JP, Fontaine G, Gear K, Hauer R, Nava A, Picard MH, Protonotarios N, Saffitz JE, Sanborn DMY, Steinberg JS, Tandri H, Thiene G, Towbin JA, Tsatsopoulou A, Wichter T, Zareba W. Diagnosis of Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia: Proposed Modification of the Task Force Criteria. Circulation. 2010;121:1533–1541. - PMC - PubMed
-
- Corrado D, Wichter T, Link MS, Hauer RNW, Marchlinski FE, Anastasakis A, Bauce B, Basso C, Brunckhorst C, Tsatsopoulou A, Tandri H, Paul M, Schmied C, Pelliccia A, Duru F, Protonotarios N, Estes NM, McKenna WJ, Thiene G, Marcus FI, Calkins H. Treatment of Arrhythmogenic Right Ventricular Cardiomyopathy/Dysplasia: An International Task Force Consensus Statement. American Heart Association Journals. 2015:441–453.
-
- Basso C, Thiene G, Corrado D, Angelini A, Nava A, Valente M. Arrhythmogenic right ventricular cardiomyopathy. Dysplasia, dystrophy, or myocarditis? Circulation. 1996;94:983–991. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
