

Evidence from high-altitude acclimatization for an integrated cerebrovascular and ventilatory hypercapnic response but different responses to hypoxia
- PMID: 28705997
- PMCID: PMC6734088
- DOI: 10.1152/japplphysiol.00341.2017
Evidence from high-altitude acclimatization for an integrated cerebrovascular and ventilatory hypercapnic response but different responses to hypoxia
Abstract
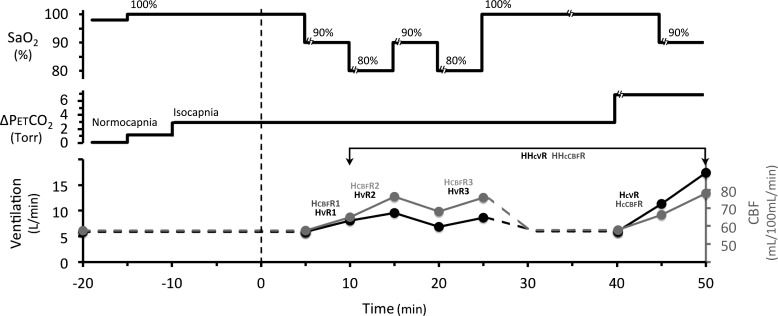
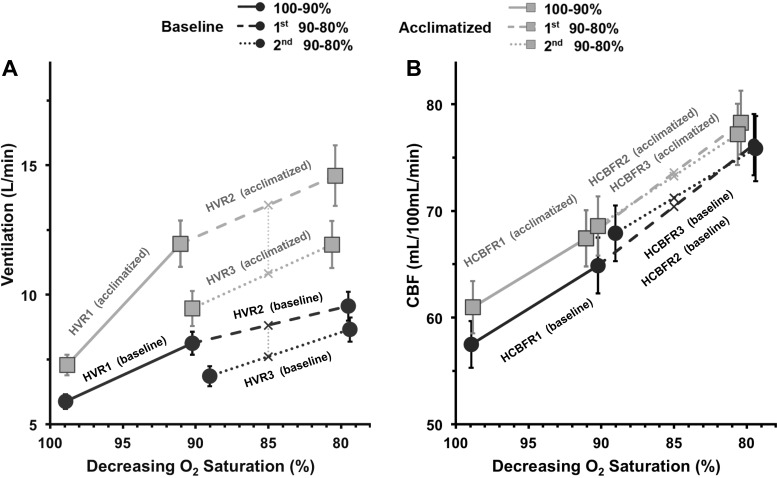
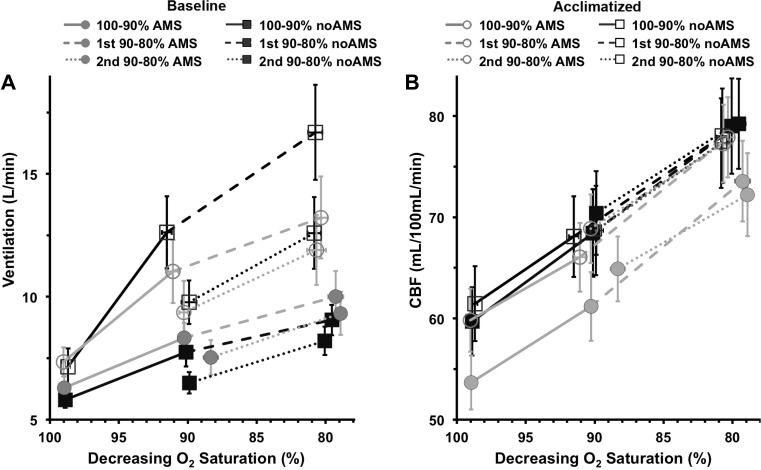
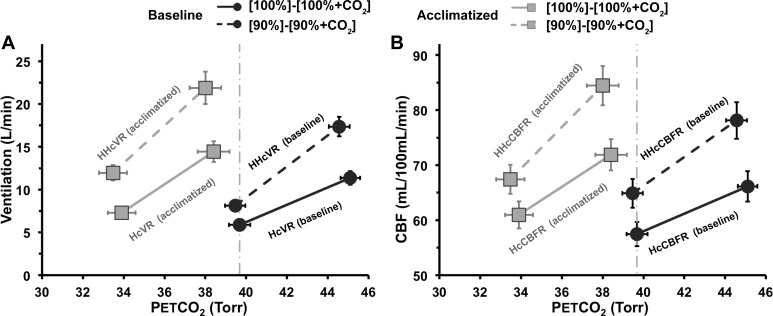
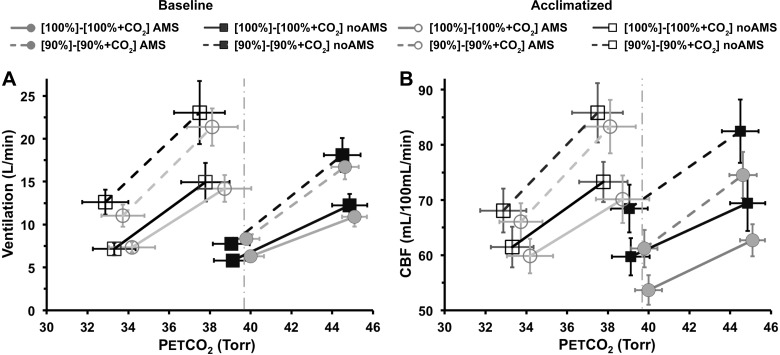
Ventilation and cerebral blood flow (CBF) are both sensitive to hypoxia and hypercapnia. To compare chemosensitivity in these two systems, we made simultaneous measurements of ventilatory and cerebrovascular responses to hypoxia and hypercapnia in 35 normal human subjects before and after acclimatization to hypoxia. Ventilation and CBF were measured during stepwise changes in isocapnic hypoxia and iso-oxic hypercapnia. We used MRI to quantify actual cerebral perfusion. Measurements were repeated after 2 days of acclimatization to hypoxia at 3,800 m altitude (partial pressure of inspired O2 = 90 Torr) to compare plasticity in the chemosensitivity of these two systems. Potential effects of hypoxic and hypercapnic responses on acute mountain sickness (AMS) were assessed also. The pattern of CBF and ventilatory responses to hypercapnia were almost identical. CO2 responses were augmented to a similar degree in both systems by concomitant acute hypoxia or acclimatization to sustained hypoxia. Conversely, the pattern of CBF and ventilatory responses to hypoxia were markedly different. Ventilation showed the well-known increase with acute hypoxia and a progressive decline in absolute value over 25 min of sustained hypoxia. With acclimatization to hypoxia for 2 days, the absolute values of ventilation and O2 sensitivity increased. By contrast, O2 sensitivity of CBF or its absolute value did not change during sustained hypoxia for up to 2 days. The results suggest a common or integrated control mechanism for CBF and ventilation by CO2 but different mechanisms of O2 sensitivity and plasticity between the systems. Ventilatory and cerebrovascular responses were the same for all subjects irrespective of AMS symptoms. NEW & NOTEWORTHY Ventilatory and cerebrovascular hypercapnic response patterns show similar plasticity in CO2 sensitivity following hypoxic acclimatization, suggesting an integrated control mechanism. Conversely, ventilatory and cerebrovascular hypoxic responses differ. Ventilation initially increases but adapts with prolonged hypoxia (hypoxic ventilatory decline), and ventilatory sensitivity increases following acclimatization. In contrast, cerebral blood flow hypoxic sensitivity remains constant over a range of hypoxic stimuli, with no cerebrovascular acclimatization to sustained hypoxia, suggesting different mechanisms for O2 sensitivity in the two systems.
Keywords: acute mountain sickness; cerebral blood flow; high altitude; hypoxia; hypoxic ventilatory response; magnetic resonance imaging.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
References
-
- Berger MG, Vandier C, Bonnet P, Jackson WF, Rusch NJ. Intracellular acidosis differentially regulates KV channels in coronary and pulmonary vascular muscle. Am J Physiol 275: H1351–H1359, 1998. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources