

Cross-sectional study of the hospital management of adult patients with a suspected seizure (EPIC2)
- PMID: 28706099
- PMCID: PMC5541576
- DOI: 10.1136/bmjopen-2016-015696
Cross-sectional study of the hospital management of adult patients with a suspected seizure (EPIC2)
Abstract
Objective: To determine the clinical characteristics, management and outcomes of patients taken to hospital by emergency ambulance after a suspected seizure.
Design: Quantitative cross-sectional retrospective study of a consecutive series of patients.
Setting: An acute hospital trust in a large city in England.
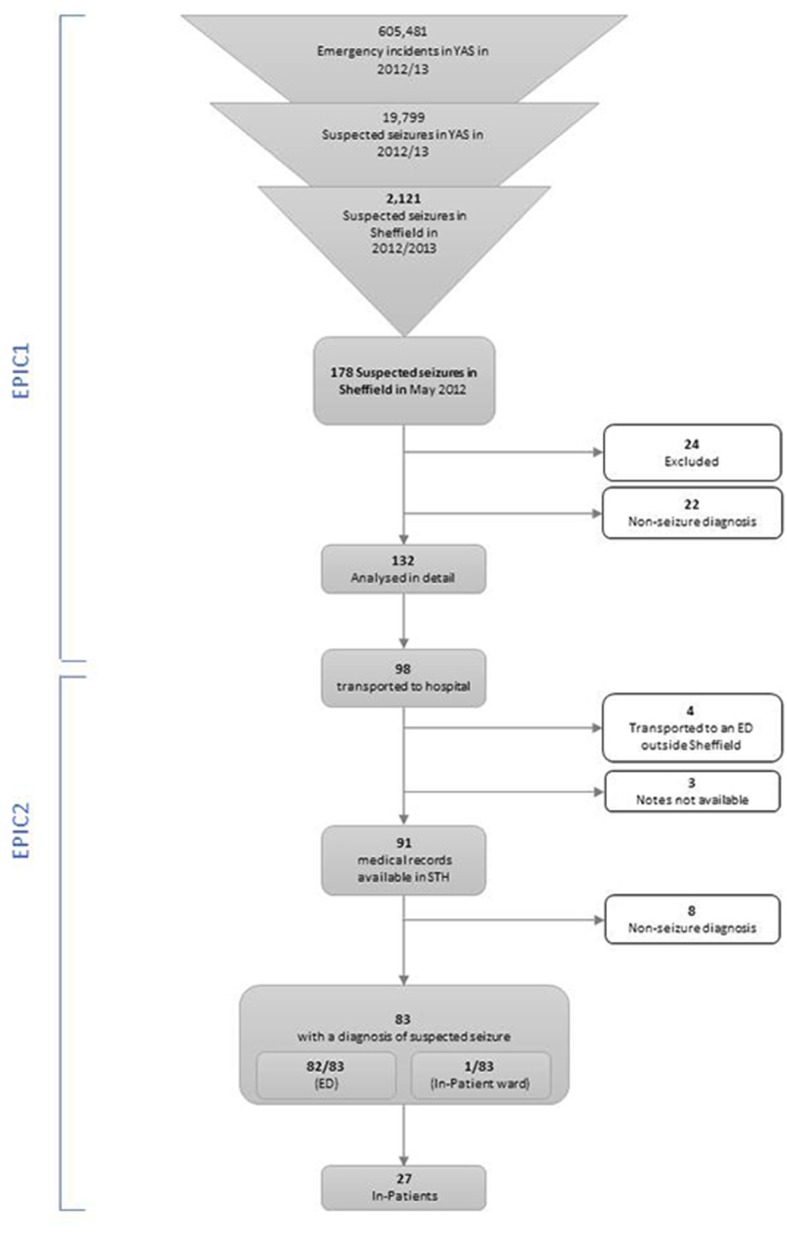
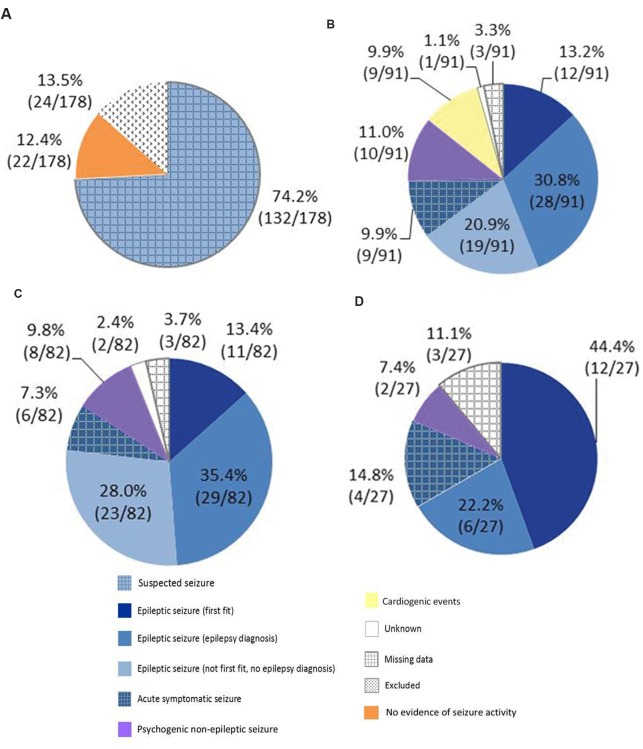
Participants: In 2012-2013, the regions' ambulance service managed 605 481 emergency incidents, 74 141/605 481 originated from Sheffield (a large city in the region), 2121/74 141 (2.9%) were suspected seizures and 178/2121 occurred in May 2012. We undertook detailed analysis of the medical records of the 91/178 patients who were transported to the city's acute hospital. After undertaking a retrospective review of the medical records, the best available aetiological explanation for the seizures was determined.
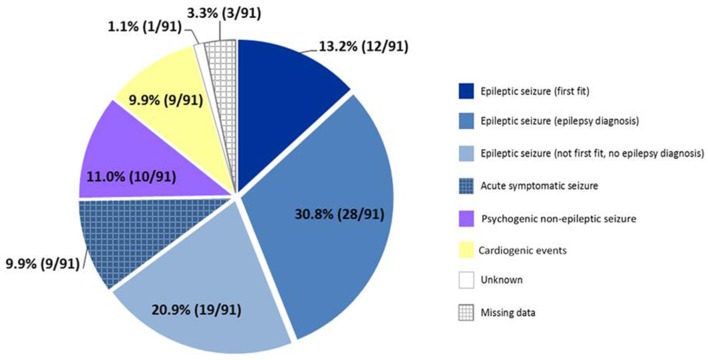
Results: The best available aetiological explanation for 74.7% (68/91) of the incidents was an epileptic seizure, 11.0% (10/91) were psychogenic non-epileptic seizures and 9.9% (9/91) were cardiogenic events. The epileptic seizures fall into the following four categories: first epileptic seizure (13.2%, 12/91), epileptic seizure with a historical diagnosis of epilepsy (30.8%, 28/91), recurrent epileptic seizures without a historical diagnosis of epilepsy (20.9%, 19/91) and acute symptomatic seizures (9.9%, 9/91). Of those with seizures (excluding cardiogenic events), 2.4% (2/82) of patients were seizing on arrival in the Emergency Department (ED), 19.5% (16/82) were postictal and 69.5% (57/82) were alert. 63.4% (52/82) were discharged at the end of their ED attendance and 36.5% (19/52) of these had no referral or follow-up.
Conclusions: Most suspected seizures are epileptic seizures but this is a diagnostically heterogeneous group. Only a small minority of patients require emergency medical care but most are transported to hospital. Few patients receive expert review and many are discharged home without referral to a specialist leaving them at risk of further seizures and the associated morbidity, mortality and health services costs of poorly controlled epilepsy.
Keywords: Epilepsy; Neurology.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: JMD received a grant of £3500 in 2014 from UCB Pharma Limited (paid to The University of Sheffield) to study unscheduled admissions for seizures using Hospital Episode Statistics. UCB had no direct input into the project. The other authors have no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases