

Hypertrophic Olivary Degeneration and Palatal or Oculopalatal Tremor
- PMID: 28706504
- PMCID: PMC5490180
- DOI: 10.3389/fneur.2017.00302
Hypertrophic Olivary Degeneration and Palatal or Oculopalatal Tremor
Abstract
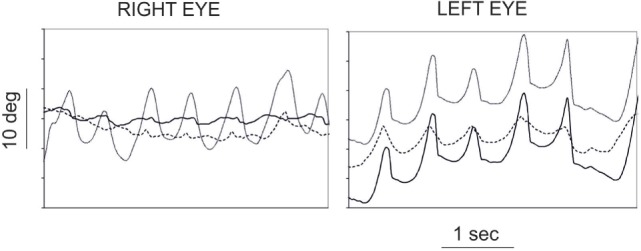
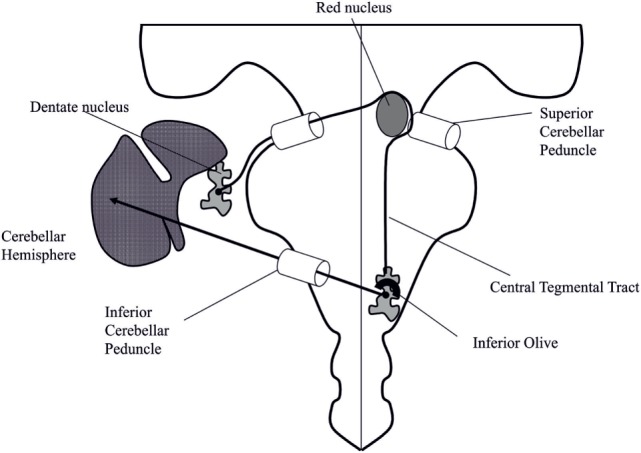
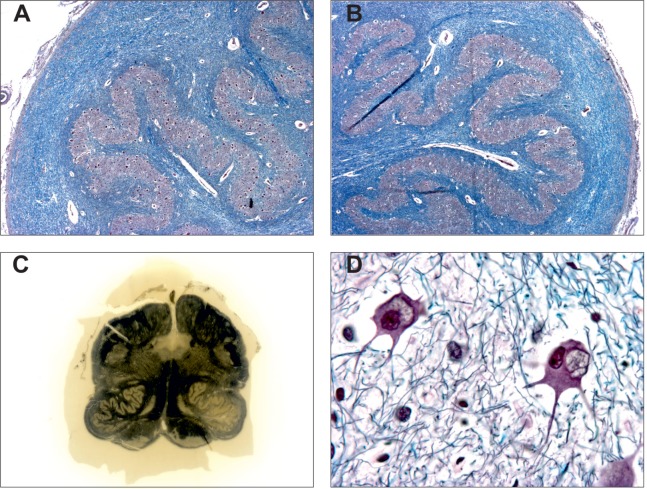
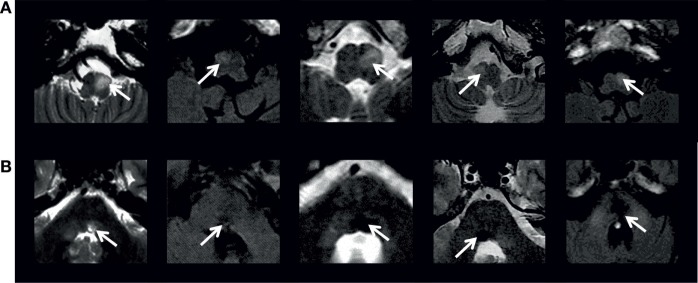
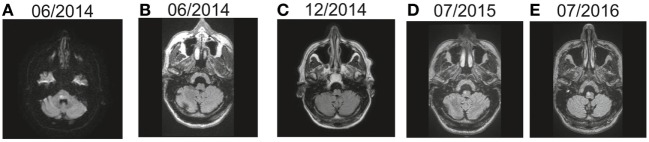
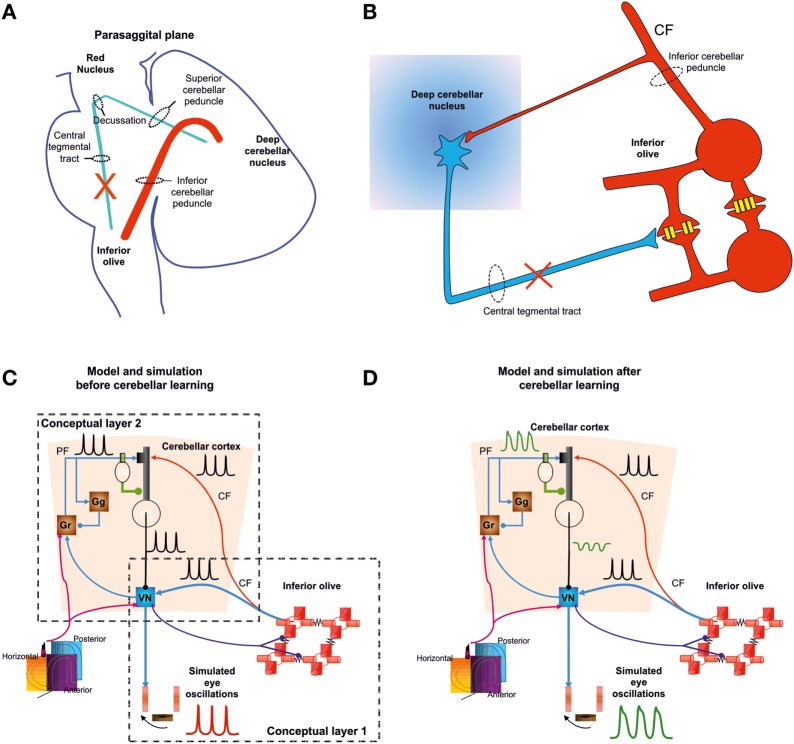
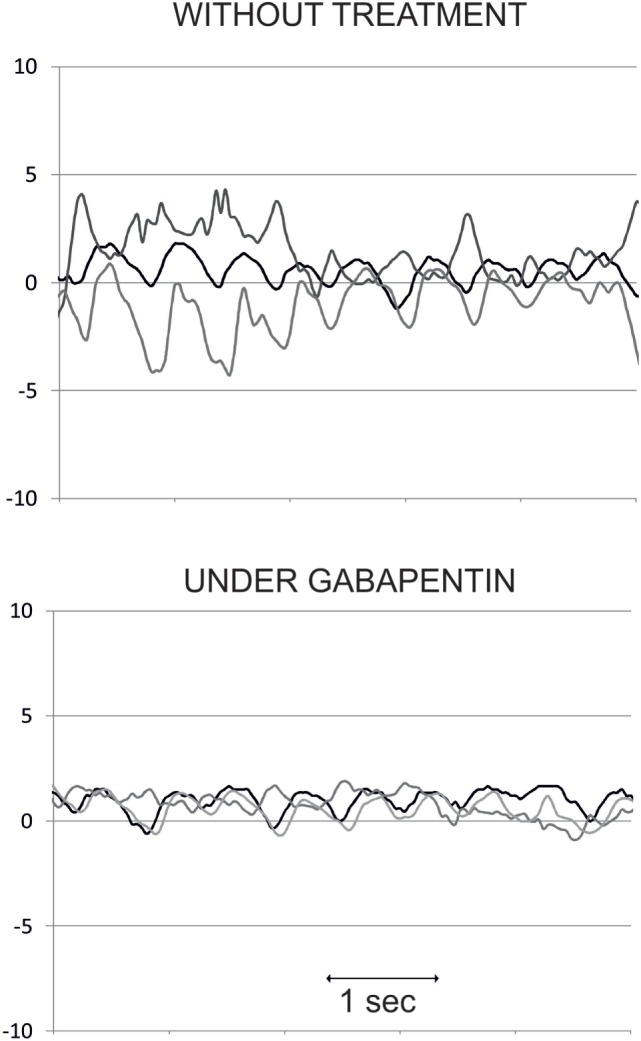
Hypertrophic degeneration of the inferior olive is mainly observed in patients developing palatal tremor (PT) or oculopalatal tremor (OPT). This syndrome manifests as a synchronous tremor of the palate (PT) and/or eyes (OPT) that may also involve other muscles from the branchial arches. It is associated with hypertrophic inferior olivary degeneration that is characterized by enlarged and vacuolated neurons, increased number and size of astrocytes, severe fibrillary gliosis, and demyelination. It appears on MRI as an increased T2/FLAIR signal intensity and enlargement of the inferior olive. There are two main conditions in which hypertrophic degeneration of the inferior olive occurs. The most frequent, studied, and reported condition is the development of PT/OPT and hypertrophic degeneration of the inferior olive in the weeks or months following a structural brainstem or cerebellar lesion. This "symptomatic" condition requires a destructive lesion in the Guillain-Mollaret pathway, which spans from the contralateral dentate nucleus via the brachium conjunctivum and the ipsilateral central tegmental tract innervating the inferior olive. The most frequent etiologies of destructive lesion are stroke (hemorrhagic more often than ischemic), brain trauma, brainstem tumors, and surgical or gamma knife treatment of brainstem cavernoma. The most accepted explanation for this symptomatic PT/OPT is that denervated olivary neurons released from inhibitory inputs enlarge and develop sustained synchronized oscillations. The cerebellum then modulates/accentuates this signal resulting in abnormal motor output in the branchial arches. In a second condition, PT/OPT and progressive cerebellar ataxia occurs in patients without structural brainstem or cerebellar lesion, other than cerebellar atrophy. This syndrome of progressive ataxia and palatal tremor may be sporadic or familial. In the familial form, where hypertrophic degeneration of the inferior olive may not occur (or not reported), the main reported etiologies are Alexander disease, polymerase gamma mutation, and spinocerebellar ataxia type 20. Whether or not these are associated with specific degeneration of the dentato-olivary pathway remain to be determined. The most symptomatic consequence of OPT is eye oscillations. Therapeutic trials suggest gabapentin or memantine as valuable drugs to treat eye oscillations in OPT.
Keywords: Guillain–Mollaret triangle; dentato–olivary pathway; hypertrophic degeneration of inferior olive; pendular nystagmus; progressive ataxia and palatal tremor; symptomatic palatal tremor.
Figures
Similar articles
-
Hypertrophic olivary degeneration: A case report.Indian J Radiol Imaging. 2019 Oct-Dec;29(4):435-437. doi: 10.4103/ijri.IJRI_412_18. Epub 2019 Dec 31. Indian J Radiol Imaging. 2019. PMID: 31949348 Free PMC article.
-
Bilateral Hypertrophic Olivary Degeneration Following Brainstem Insult: A Retrospective Review and Examination of Causative Pathology.Neurosci Insights. 2021 Apr 30;16:26331055211007445. doi: 10.1177/26331055211007445. eCollection 2021. Neurosci Insights. 2021. PMID: 34485912 Free PMC article. Review.
-
Hypertrophic olivary degeneration and palatal myoclonus from a Streptococcus intermedius infection of the brain: illustrative case.J Neurosurg Case Lessons. 2022 Jun 13;3(24):CASE2265. doi: 10.3171/CASE2265. eCollection 2022 Jun 13. J Neurosurg Case Lessons. 2022. PMID: 35733632 Free PMC article.
-
The dentato-rubro-olivary tract: clinical dimension of this anatomical pathway.Case Rep Otolaryngol. 2013;2013:934386. doi: 10.1155/2013/934386. Epub 2013 Apr 11. Case Rep Otolaryngol. 2013. PMID: 23662232 Free PMC article.
-
Progressive ataxia and palatal tremor (PAPT): clinical and MRI assessment with review of palatal tremors.Brain. 2004 Jun;127(Pt 6):1252-68. doi: 10.1093/brain/awh137. Epub 2004 Apr 16. Brain. 2004. PMID: 15090471 Review.
Cited by
-
Palatal Tremor - Pathophysiology, Clinical Features, Investigations, Management and Future Challenges.Tremor Other Hyperkinet Mov (N Y). 2020 Oct 8;10:40. doi: 10.5334/tohm.188. Tremor Other Hyperkinet Mov (N Y). 2020. PMID: 33101766 Free PMC article. Review.
-
Effect of convergence on the horizontal VOR in normal subjects and patients with peripheral and central vestibulopathy.Neurol Sci. 2022 Jul;43(7):4519-4529. doi: 10.1007/s10072-022-05970-8. Epub 2022 Mar 4. Neurol Sci. 2022. PMID: 35246817
-
Oncologic causes of oculopalatal tremors: neurophysiology and treatment.Acta Neurol Belg. 2021 Oct;121(5):1111-1116. doi: 10.1007/s13760-021-01761-8. Epub 2021 Jul 20. Acta Neurol Belg. 2021. PMID: 34286476 Review.
-
Autosomal recessive cerebellar ataxias: a diagnostic classification approach according to ocular features.Front Integr Neurosci. 2024 Feb 7;17:1275794. doi: 10.3389/fnint.2023.1275794. eCollection 2023. Front Integr Neurosci. 2024. PMID: 38390227 Free PMC article.
-
High-Frequency Palatal Tremor and Stimulus-Sensitive Leg Myoclonus with Degeneration of Inferior Olivary Nuclei in Celiac Disease.Mov Disord Clin Pract. 2020 Sep 29;7(Suppl 3):S93-S95. doi: 10.1002/mdc3.13079. eCollection 2020 Sep. Mov Disord Clin Pract. 2020. PMID: 33015235 Free PMC article. No abstract available.
References
-
- Oppenheim H. Über ein bei Krankheitsprocessen in der hinteren Schadelgrube beobachtetes symptom. Neurol Zbl (1889) 8:132–4.
-
- Spencer HR. Pharyngeal and laryngeal “nystagmus”. Lancet (1886) 2:702.10.1016/S0140-6736(01)78357-2 - DOI
-
- Van Bogaert L, Bertrand I. Sur les myoclonies associées synchrones et rythmiques par lésion en foyer du tronc cérébral. Rev Neurol (1928) 1(2):203.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources