

Endotype-driven treatment in chronic upper airway diseases
- PMID: 28706720
- PMCID: PMC5506670
- DOI: 10.1186/s13601-017-0157-8
Endotype-driven treatment in chronic upper airway diseases
Abstract
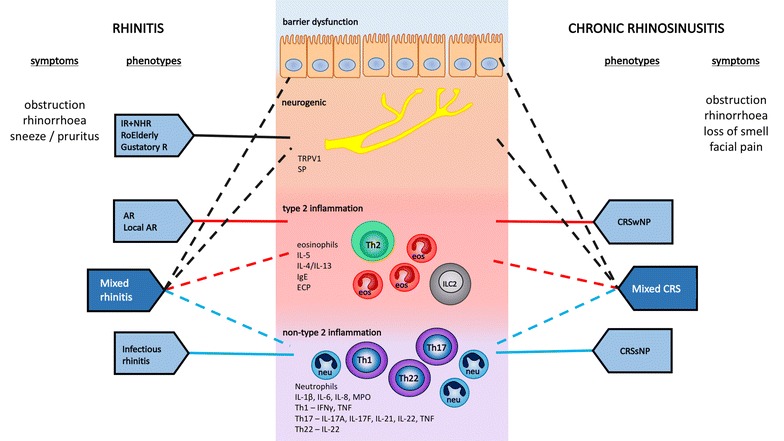
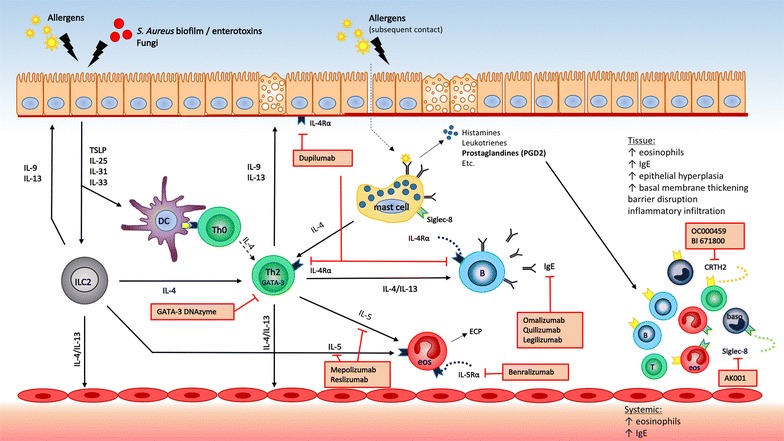
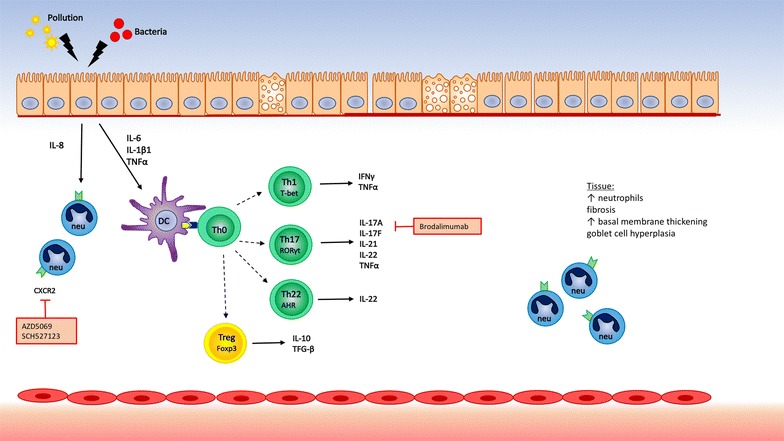
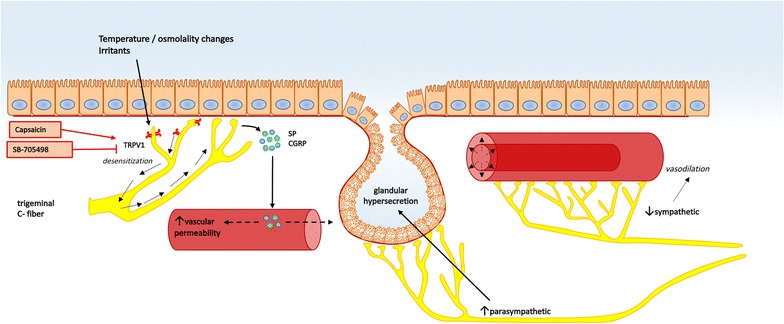
Rhinitis and rhinosinusitis are the two major clinical entities of chronic upper airway disease. Chronic rhinosinusitis (CRS) and allergic rhinitis (AR) affect respectively up to 10 and 30% of the total population, hence being associated with an important socio-economic burden. Different phenotypes of rhinitis and CRS have been described based on symptom severity and duration, atopy status, level of control, comorbidities and presence or absence of nasal polyps in CRS. The underlying pathophysiological mechanisms are diverse, with different, and sometimes overlapping, endotypes being recognized. Type 2 inflammation is well characterized in both AR and CRS with nasal polyps (CRSwNP), whereas type 1 inflammation is found in infectious rhinitis and CRS without nasal polyps (CRSsNP). The neurogenic endotype has been demonstrated in some forms of non-allergic rhinitis. Epithelial barrier dysfunction is shown in AR and CRSwNP. Emerging therapies are targeting one specific pathophysiological pathway or endotype. This endotype-driven treatment approach requires careful selection of the patient population who might benefit from a specific treatment. Personalized medicine is addressing the issue of providing targeted treatment for the right patient and should be seen as one aspect of the promising trend towards precision medicine. This review provides a comprehensive overview of the current state of endotypes, biomarkers and targeted treatments in chronic inflammatory conditions of the nose and paranasal sinuses.
Keywords: Biologicals; Biomarker; Chronic rhinosinusitis; Personalised medicine; Phenotype; Precision medicine; Rhinitis.
Figures
References
-
- Muraro A, Fokkens WJ, Pietikainen S, Borrelli D, Agache I, Bousquet J, et al. European symposium on precision medicine in allergy and airways diseases: report of the European Union parliament symposium (October 14, 2015) Rhinology. 2015;53(4):303–307. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
