

Impact of Cold Ischemia Time in Kidney Transplants From Donation After Circulatory Death Donors
- PMID: 28706980
- PMCID: PMC5498018
- DOI: 10.1097/TXD.0000000000000680
Impact of Cold Ischemia Time in Kidney Transplants From Donation After Circulatory Death Donors
Abstract
Background: Deceased-donor kidneys are exposed to ischemic events from donor instability during the process of donation after circulatory death (DCD). Clinicians may be reluctant to transplant DCD kidneys with prolonged cold ischemia time (CIT) for fear of an additional deleterious effect.
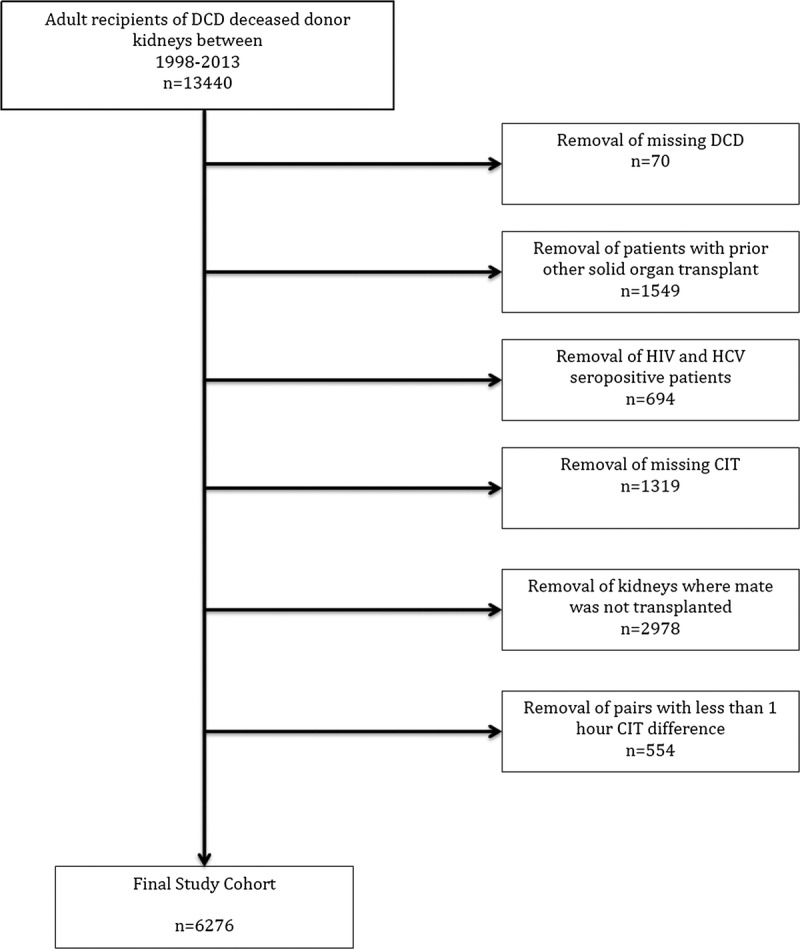
Methods: We performed a retrospective cohort study examining US registry data between 1998 and 2013 of adult first-time kidney-only recipients of paired kidneys (derived from the same donor transplanted into different recipients) from DCD donors.
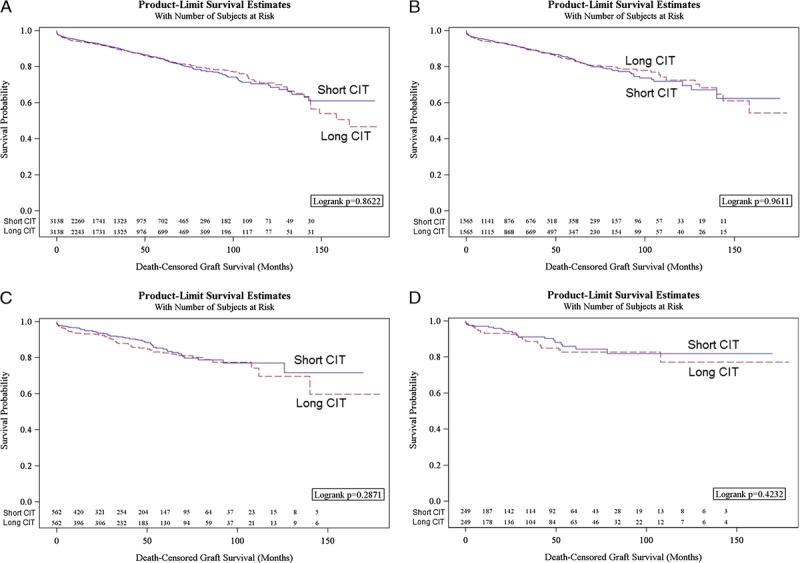
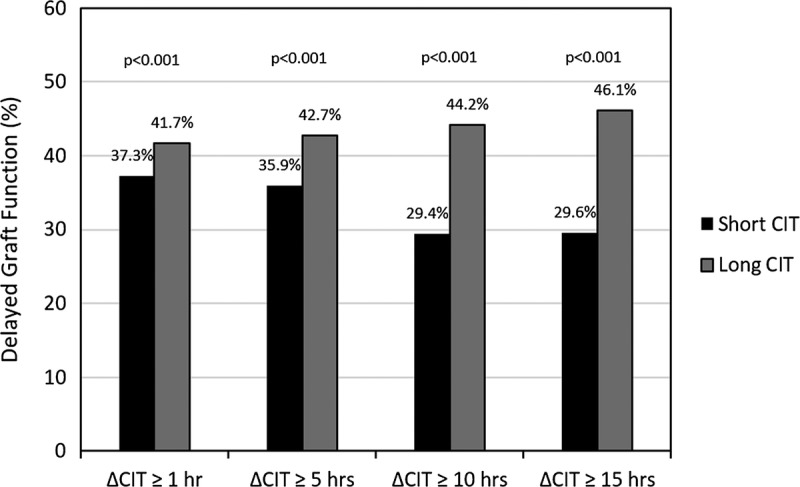
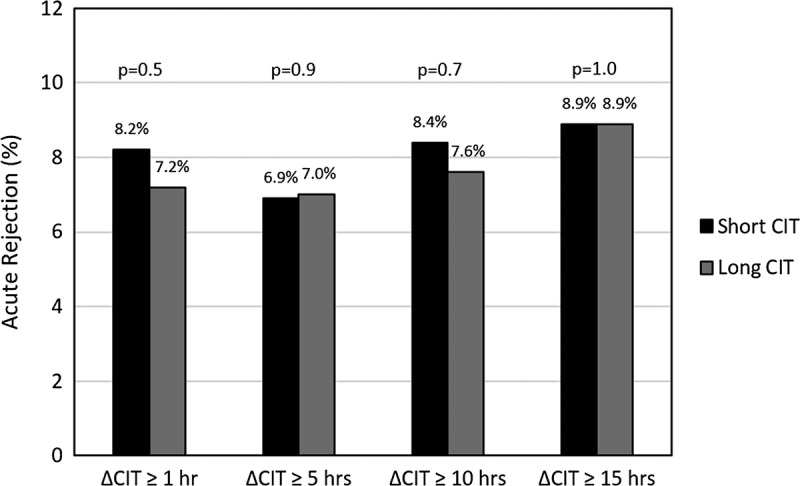
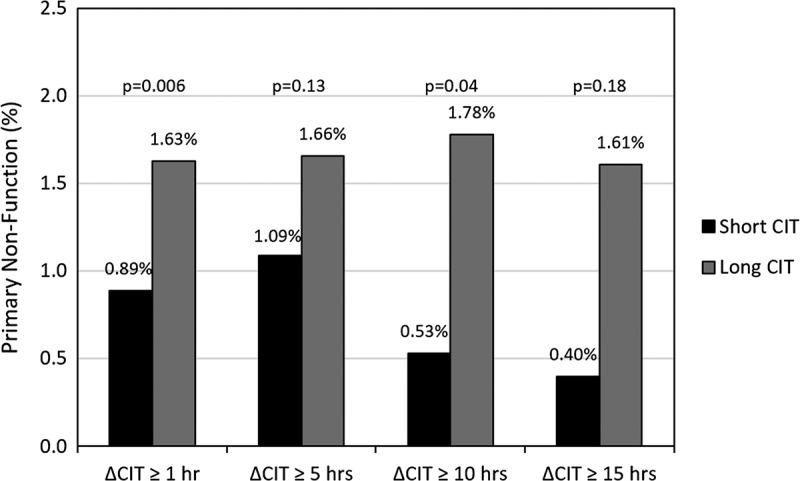
Results: On multivariable analysis, death-censored graft survival (DCGS) was comparable between recipients of kidneys with higher CIT relative to paired donor recipients with lower CIT when the CIT difference was 1 hour or longer (adjusted hazard ratio, [aHR], 1.02; 95% confidence interval [CI], 0.88-1.17; n = 6276), 5 hours or longer (aHR, 0.98; 95% CI, 0.80-1.19; n = 3130), 10 hours or longer (aHR, 1.15; 95% CI, 0.82-1.60; n = 1124) or 15 hours (aHR, 1.15; 95% CI, 0.66-1.99; n = 498). There was a higher rate of primary non function in the long CIT groups for delta 1 hour or longer (0.89% vs 1.63%; P = 0.006), 5 hours (1.09% vs 1.67%, P = 0.13); 10 hours (0.53% vs 1.78%; P = 0.03), and 15 hours (0.40% vs 1.61%; P = 0.18), respectively. Between each of the 4 delta CIT levels of shorter and longer CIT, there was a significantly and incrementally higher rate of delayed graft function in the long CIT groups for delta 1 hour or longer (37.3% vs 41.7%; P < 0.001), 5 hours (35.9% vs 42.7%; P < 0.001), 10 hours (29.4% vs 44.2%, P < 0.001), and 15 hours (29.6% vs 46.1%, P < 0.001), respectively. Overall patient survival was comparable with delta CITs of 1 hour or longer (aHR, 0.96; 95% CI, 0.84-1.08), 5 hours (aHR, 1.01; 95% CI, 0.85-1.20), and 15 hours (aHR, 1.27; 95% CI, 0.79-2.06) but not 10 hours (aHR, 1.47; 95% CI, 1.09-1.98).
Conclusions: These results suggest that in the setting of a prior ischemic donor event, prolonged CIT has limited bearing on long-term outcomes.
Conflict of interest statement
The authors declare no funding or conflicts of interest.
Figures
References
-
- Shapiro R, Halloran PF, Delmonico FL, et al. The “two, one, zero” decision: what to do with suboptimal deceased donor kidneys. Am J Transplant. 2010;10:1959–1960. - PubMed
-
- Massie AB, Desai NM, Montgomery RA, et al. Improving distribution efficiency of hard-to-place deceased donor kidneys: predicting probability of discard or delay. Am J Transplant. 2010;10:1613–1620. - PubMed
-
- Summers DM, Johnson RJ, Hudson A, et al. Effect of donor age and cold storage time on outcome in recipients of kidneys donated after circulatory death in the UK: a cohort study. Lancet. 2013;381:727–734. - PubMed
-
- Locke JE, Segev DL, Warren DS, et al. Outcomes of kidneys from donors after cardiac death: implications for allocation and preservation. Am J Transplant. 2007;7:1797–1807. - PubMed
-
- Opelz G, Döhler B. Multicenter analysis of kidney preservation. Transplantation. 2007;83:247–253. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
