

What Factors are Associated With 90-day Episode-of-care Payments for Younger Patients With Total Joint Arthroplasty?
- PMID: 28707110
- PMCID: PMC5638736
- DOI: 10.1007/s11999-017-5444-0
What Factors are Associated With 90-day Episode-of-care Payments for Younger Patients With Total Joint Arthroplasty?
Abstract
Background: Total joint arthroplasty (TJA) has been identified as a procedure with substantial variations in inpatient and postacute care payments. Most studies in this area have focused primarily on the Medicare population and rarely have characterized the younger commercially insured populations. Understanding the inpatient and postdischarge care service-component differences across 90-day episodes of care and factors associated with payments for younger patients is crucial for successful implementation of bundled payments in TJA in non-Medicare populations.
Purpose: (1) To assess the mean total payment for a 90-day primary TJA episode, including the proportion attributable to postdischarge care, and (2) to evaluate the role of procedure, patient, and hospital-level factors associated with 90-day episode-of-care payments in a non-Medicare patient population younger than 65 years.
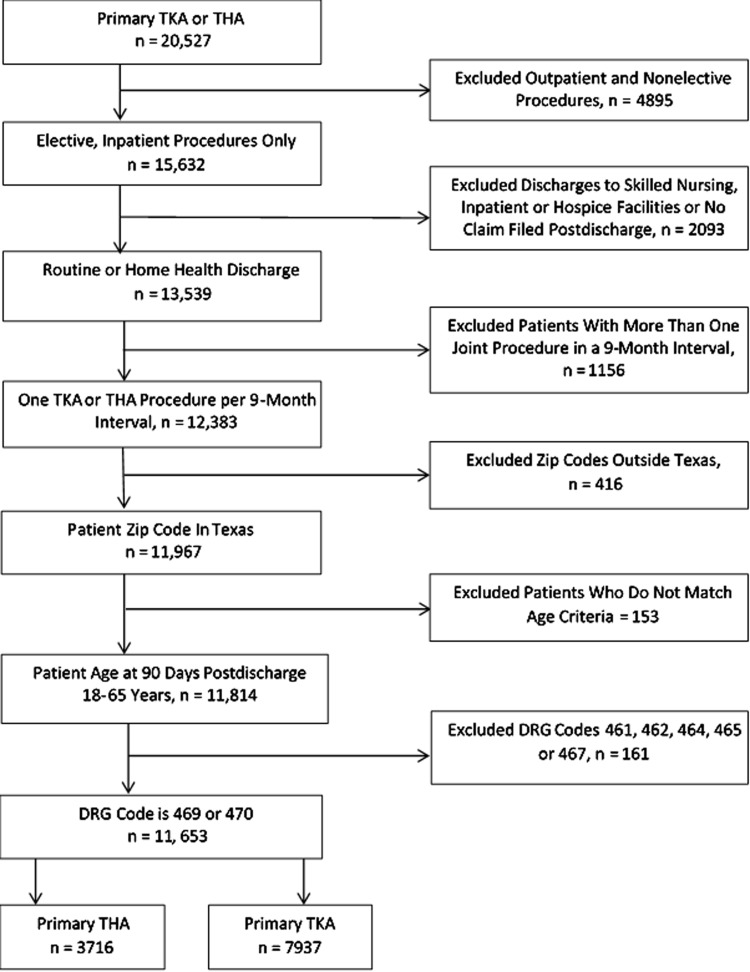
Method: Claims data for 2008 to 2013 from Blue Cross Blue Shield of Texas were obtained for primary TJAs. A total of 11,131 procedures were examined by aggregating payments for the index hospital stay and any postacute care including rehabilitation services and unplanned readmissions during the 90-day postdischarge followup period. A three-level hierarchical model was developed to determine procedure-, patient-, and hospital-level factors associated with 90-day episode-of-care payments.
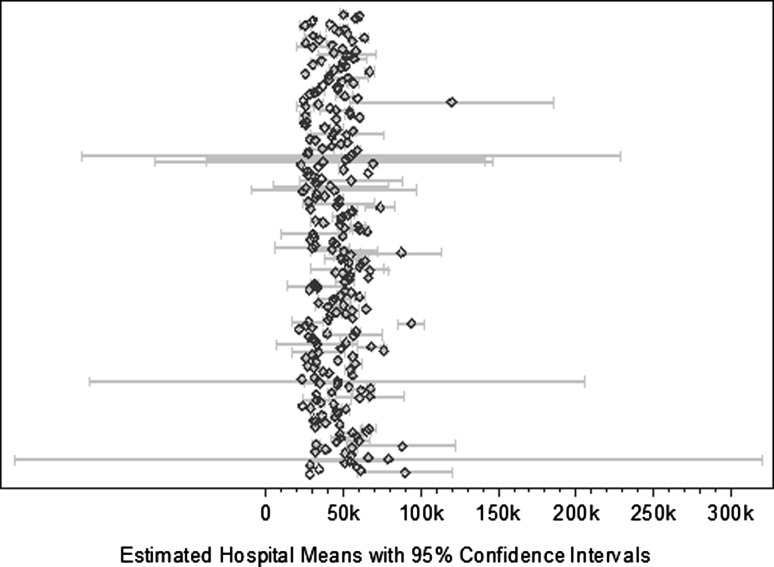
Results: The mean total payment for a 90-day episode for TJA was USD 47,700 adjusted to 2013 USD. Only 14% of 90-day episode payments in our population was attributable to postdischarge-care services, which is substantially lower than the percentage estimated in the Medicare population. A prolonged length of stay (rate ratio [RR], 1.19; 95% CI, 1.15-1.23; p ≤ 0.001), any 90-day unplanned readmission (RR, 1.64; 95% CI, 1.57-1.71; p ≤ 0.001), computer-assisted surgery (RR, 1.031; 95% CI, 1.004-1.059; p ≤ 0.05), initial home discharge with home health component (RR, 1.029; 95% CI, 1.013-1.046; p ≤ 0.001), and very high patient morbidity burden (RR, 1.105; 95% CI, 1.062-1.150; p ≤ 0.001) were associated with increased TJA payments. Hospital-level factors associated with higher payments included urban location (RR, 1.29; 95% CI, 1.17-1.42; p ≤ 0.001), lower hospital case mix based on average relative diagnosis related group weight (RR, 0.94; 95% CI, 0.89-0.95; p ≤ 0.001), and large hospital size as defined by total discharge volume (RR, 1.082; 95% CI, 1.009-1.161; p ≤ 0.05). All procedure, patient, and hospital characterizing factors together explained 11% of variation among hospitals and 49% of variation among patients.
Conclusion: Inpatient care contributed to a much larger proportion of total payments for 90-day care episodes for primary TJA in our younger than 65-year-old commercially insured population. Thus, inpatient care will continue to be an essential target for cost-containment and delivery strategies. A high percentage of hospital-level variation in episode payments remained unexplained by hospital characteristics in our study, suggesting system inefficiencies that could be suitable for bundling. However, replication of this study among other commercial payers in other parts of the country will allow for conclusions that are more robust and generalizable.
Level of evidence: Level II, economic analysis.
Figures
Similar articles
-
Which Clinical and Patient Factors Influence the National Economic Burden of Hospital Readmissions After Total Joint Arthroplasty?Clin Orthop Relat Res. 2017 Dec;475(12):2926-2937. doi: 10.1007/s11999-017-5244-6. Clin Orthop Relat Res. 2017. PMID: 28108823 Free PMC article.
-
Are Bundled Payments a Viable Reimbursement Model for Revision Total Joint Arthroplasty?Clin Orthop Relat Res. 2016 Dec;474(12):2714-2721. doi: 10.1007/s11999-016-4953-6. Epub 2016 Jun 29. Clin Orthop Relat Res. 2016. PMID: 27357691 Free PMC article.
-
Drivers of Variation in 90-Day Episode Payments After Percutaneous Coronary Intervention.Circ Cardiovasc Interv. 2019 Jan;12(1):e006928. doi: 10.1161/CIRCINTERVENTIONS.118.006928. Circ Cardiovasc Interv. 2019. PMID: 30608883 Free PMC article.
-
Effect of Bundled Payments and Health Care Reform as Alternative Payment Models in Total Joint Arthroplasty: A Clinical Review.J Arthroplasty. 2017 Aug;32(8):2590-2597. doi: 10.1016/j.arth.2017.03.027. Epub 2017 Mar 20. J Arthroplasty. 2017. PMID: 28438453 Review.
-
Bundle Payment for Musculoskeletal Care: Current Evidence (Part 2).Orthop Clin North Am. 2018 Apr;49(2):147-156. doi: 10.1016/j.ocl.2017.11.003. Epub 2018 Feb 3. Orthop Clin North Am. 2018. PMID: 29499816 Review.
Cited by
-
Is Post-discharge Rehabilitation Timing Associated with 90-Day Readmission in Primary Total Joint Arthroplasty?HSS J. 2019 Oct;15(3):234-240. doi: 10.1007/s11420-019-09685-z. Epub 2019 Jun 15. HSS J. 2019. PMID: 31624478 Free PMC article.
-
Editor's Spotlight/Take 5-2018 John Charnley Award: Analysis of US Hip Replacement Bundled Payments: Physician-initiated Episodes Outperform Hospital-initiated Episodes.Clin Orthop Relat Res. 2019 Feb;477(2):268-270. doi: 10.1097/CORR.0000000000000626. Clin Orthop Relat Res. 2019. PMID: 30664043 Free PMC article. No abstract available.
References
-
- Berenson RA, Hoagland GW, Dranove D, Ginsberg P, Glied SA, Goldsmith J, Kocher B, Kramer WE, Levy R, McKeever DP, Pitts KB, Richman BD, Robinson JC, Roosevelt J, Rowe JW, Wolter N. Addressing Pricing Power in Health Care Markets: Principles and Policy Options to Strengthen and Shape Markets. 2015. Available at: https://www.nasi.org/research/2015/addressing-pricing-power-health-care-.... Accessed December 2, 2016.
-
- Blue Cross Blue Shield Association. The Health of America. A Study of Cost Variations for Knee and Hip Replacement Surgeries in the U.S. Available at: https://www.bcbs.com/the-health-of-america/reports/study-cost-variations.... Accessed December 11, 2016.
-
- Blue Cross Blue Shield of North Carolina. Corporate Medical Policy. Computer Assisted Surgical Navigational Orthopedic Procedures. Available at: http://www.bcbsnc.com/assets/services/public/pdfs/medicalpolicy/computer.... Accessed June 21, 2017.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
