

Imaging in Vascular Access
- PMID: 28707187
- PMCID: PMC5573761
- DOI: 10.1007/s13239-017-0317-y
Imaging in Vascular Access
Abstract
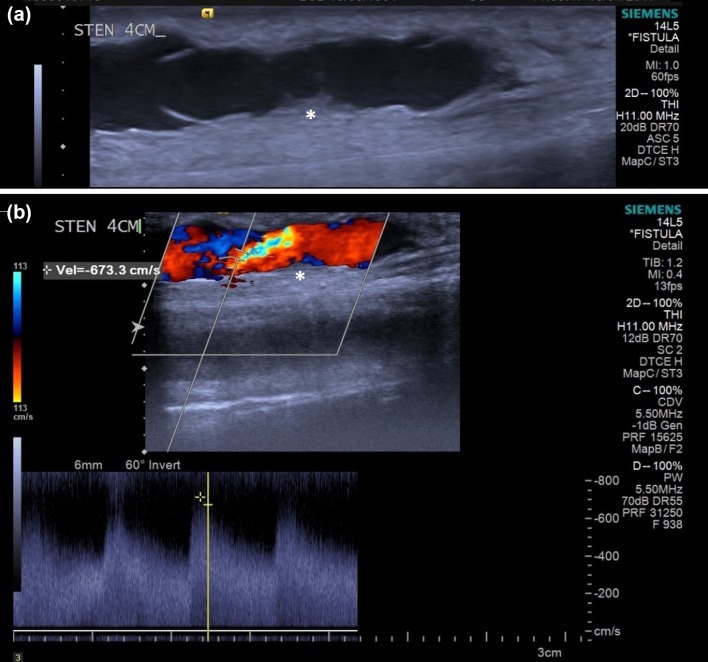
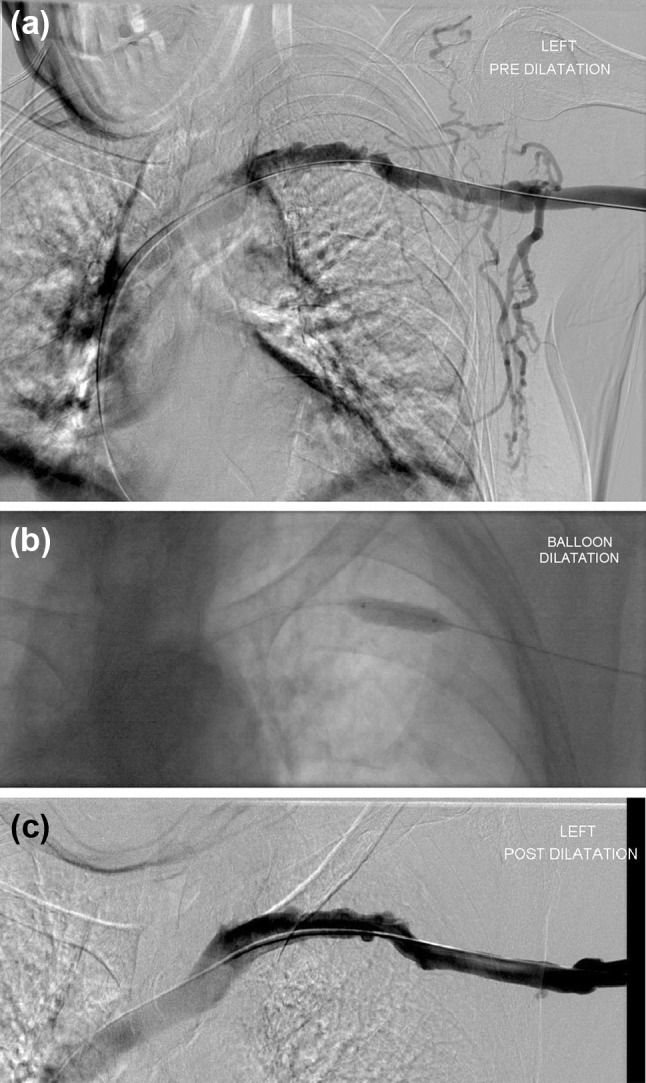
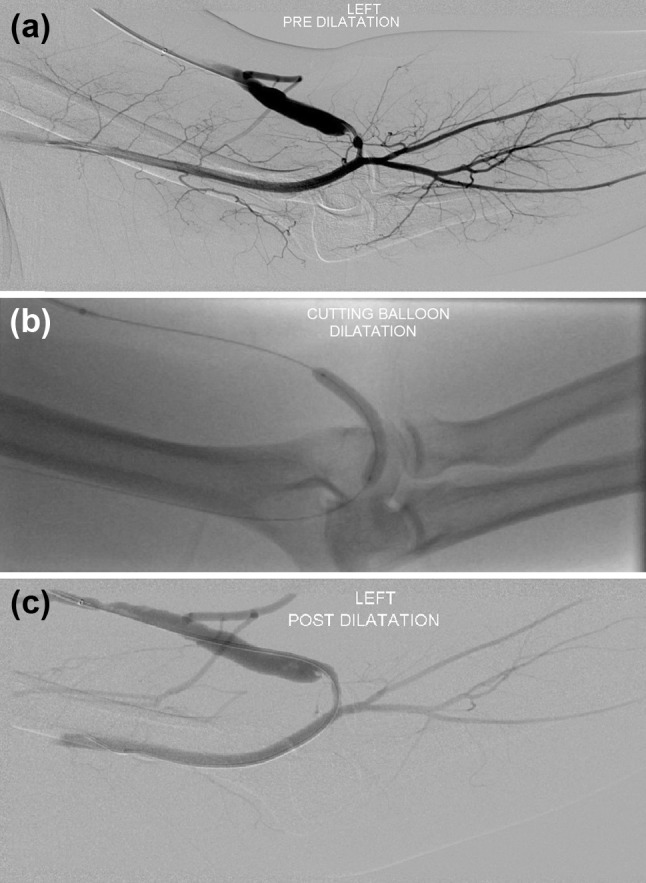
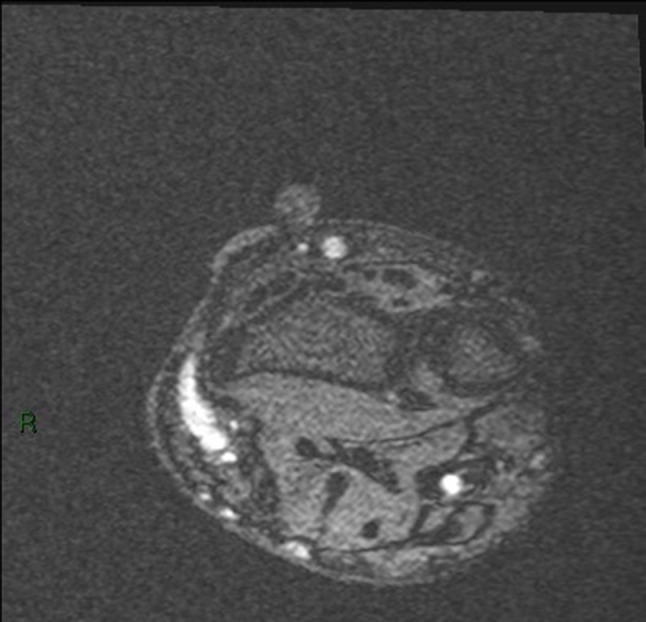
This review examines four imaging modalities; ultrasound (US), digital subtraction angiography (DSA), magnetic resonance imaging (MRI) and computed tomography (CT), that have common or potential applications in vascular access (VA). The four modalities are reviewed under their primary uses, techniques, advantages and disadvantages, and future directions that are specific to VA. Currently, US is the most commonly used modality in VA because it is cheaper (relative to other modalities), accessible, non-ionising, and does not require the use of contrast agents. DSA is predominantly only performed when an intervention is indicated. MRI is limited by its cost and the time required for image acquisition that mainly confines it to the realm of research where high resolution is required. CT's short acquisition times and high resolution make it useful as a problem-solving tool in complex cases, although accessibility can be an issue. All four imaging modalities have advantages and disadvantages that limit their use in this particular patient cohort. Current imaging in VA comprises an integrated approach with each modality providing particular uses dependent on their capabilities. MRI and CT, which currently have limited use, may have increasingly important future roles in complex cases where detailed analysis is required.
Keywords: Arteriovenous fistula; Computed tomography; Digital subtraction angiography; Magnetic resonance imaging; Medical imaging; Ultrasound; Vascular access.
Figures



References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
