

From Inflammation to Fibrosis-Molecular and Cellular Mechanisms of Myocardial Tissue Remodelling and Perspectives on Differential Treatment Opportunities
- PMID: 28707261
- PMCID: PMC5527069
- DOI: 10.1007/s11897-017-0343-y
From Inflammation to Fibrosis-Molecular and Cellular Mechanisms of Myocardial Tissue Remodelling and Perspectives on Differential Treatment Opportunities
Abstract
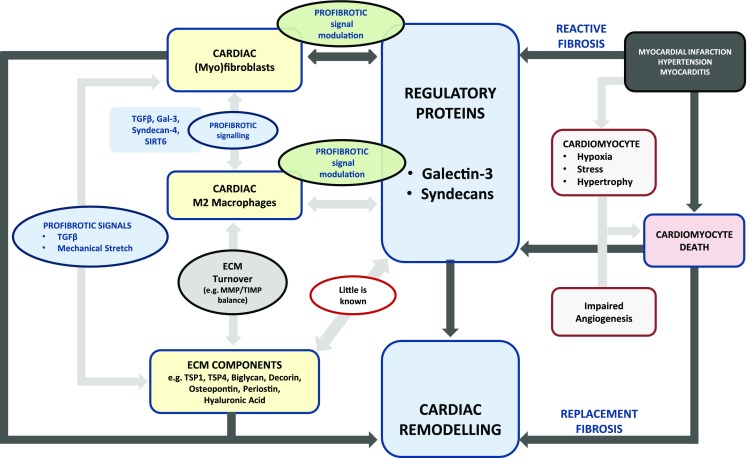
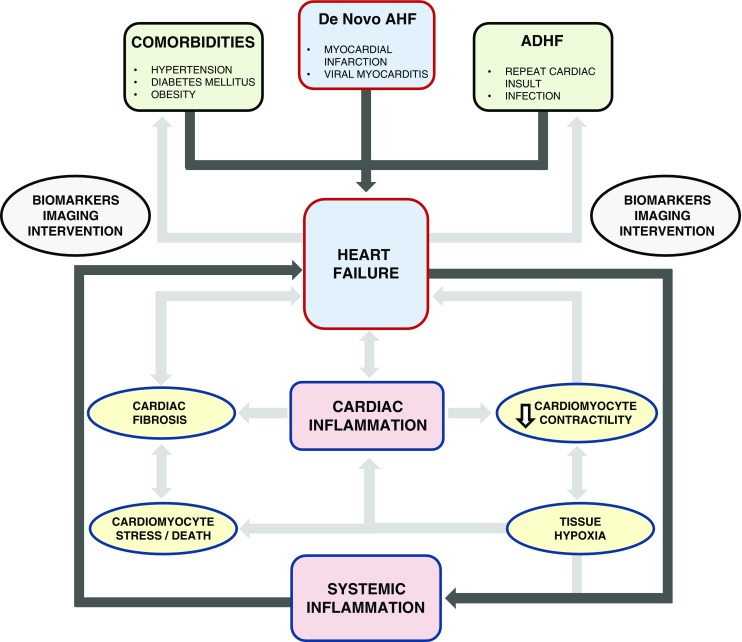
Purpose of review: In this review, we highlight the most important cellular and molecular mechanisms that contribute to cardiac inflammation and fibrosis. We also discuss the interplay between inflammation and fibrosis in various precursors of heart failure (HF) and how such mechanisms can contribute to myocardial tissue remodelling and development of HF.
Recent findings: Recently, many research articles attempt to elucidate different aspects of the interplay between inflammation and fibrosis. Cardiac inflammation and fibrosis are major pathophysiological mechanisms operating in the failing heart, regardless of HF aetiology. Currently, novel therapeutic options are available or are being developed to treat HF and these are discussed in this review. A progressive disease needs an aggressive management; however, existing therapies against HF are insufficient. There is a dynamic interplay between inflammation and fibrosis in various precursors of HF such as myocardial infarction (MI), myocarditis and hypertension, and also in HF itself. There is an urgent need to identify novel therapeutic targets and develop advanced therapeutic strategies to combat the syndrome of HF. Understanding and describing the elements of the inflammatory and fibrotic pathways are essential, and specific drugs that target these pathways need to be evaluated.
Keywords: Cardiac; ECM; Fibrosis; HF; Heart; Inflammation; Macrophages.
Conflict of interest statement
Conflict of Interest
The authors declare that they have no conflicts of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
