

Time-dependent and nonlinear effects of prognostic factors in nonmetastatic colorectal cancer
- PMID: 28707427
- PMCID: PMC5548888
- DOI: 10.1002/cam4.1116
Time-dependent and nonlinear effects of prognostic factors in nonmetastatic colorectal cancer
Abstract
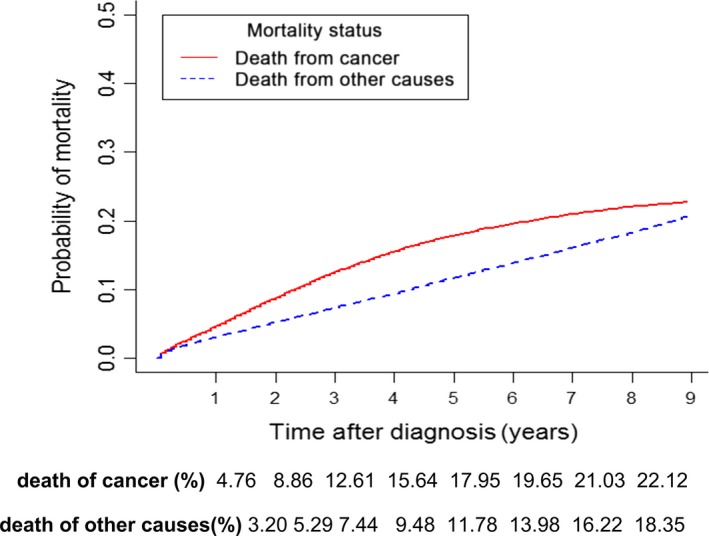
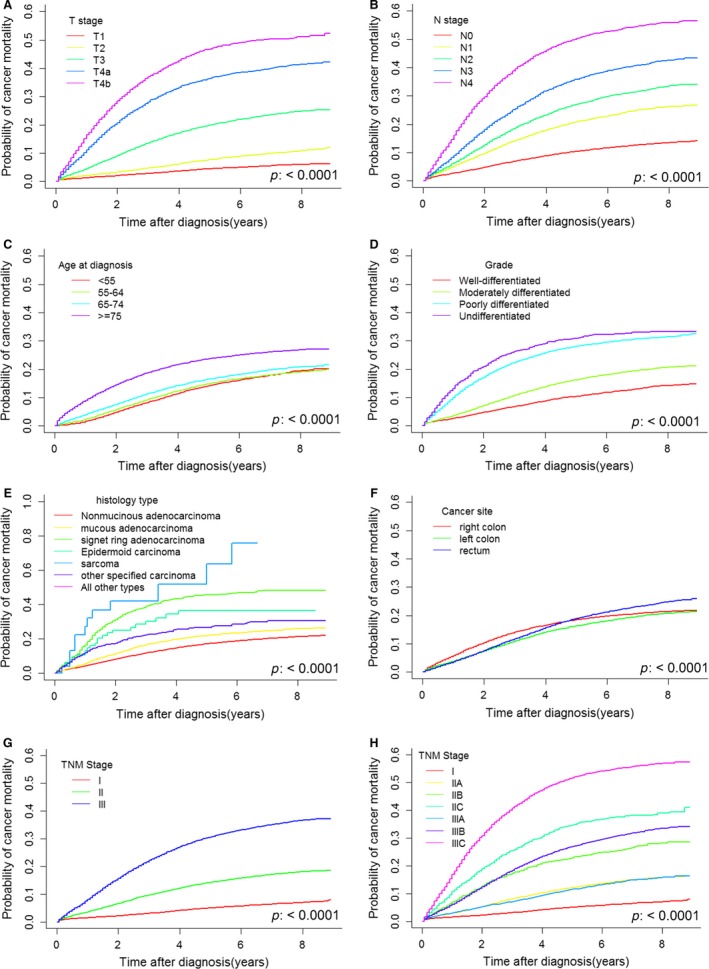
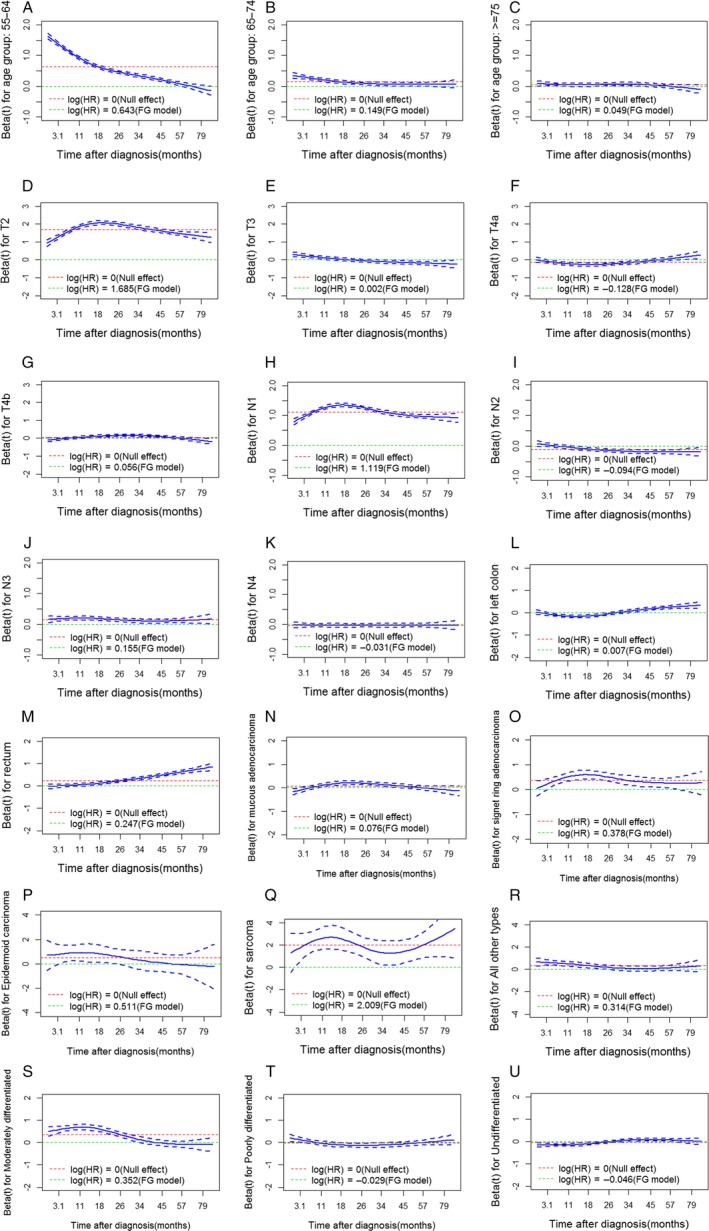
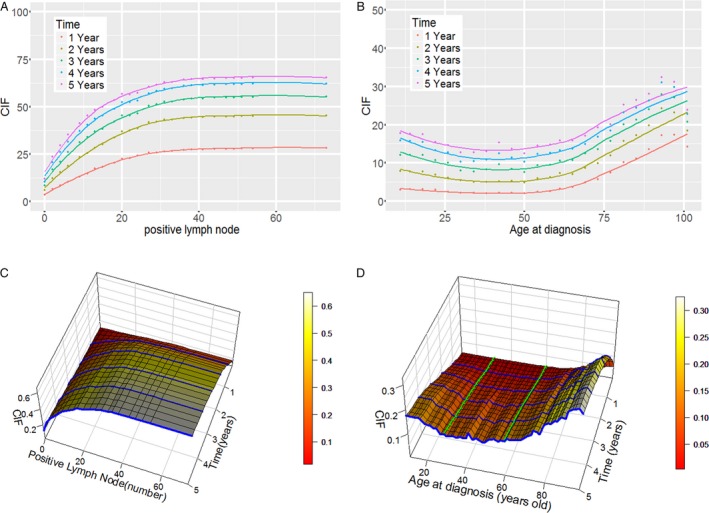
The survival risk following curative surgery for nonmetastatic colorectal cancer (CRC) may be over- or underestimated due to a lack of attention to nonlinear effects and violation of the proportional hazards assumption. In this paper, we aimed to detect and interpret the shape of time-dependent and nonlinear effects to improve the predictive performance of models of prognoses in nonmetastatic CRC patients. Data for nonmetastatic CRC patients diagnosed between 2004 and 2012 were obtained from the Surveillance Epidemiology End Results registry. Time-dependent and nonlinear effects were tested and plotted. A nonlinear model that used random survival forests was implemented. The estimated 5-year cancer-specific death rate was 17.95% (95% CI, 17.70-18.20%). Tumor invasion depth, lymph node status, age at diagnosis, tumor grade, histology and tumor site were significantly associated with cancer-specific death. Nonlinear and time-dependent effects on survival were detected. Positive lymph node number had a larger effect per unit of measurement at low values than at high values, whereas age at diagnosis showed the opposite pattern. Moreover, nonproportional hazards were detected for all covariates, indicating that the contributions of these risks to survival outcomes decreased over time. The nonlinear model predicted prognoses more accurately (C-index: 0.7934, 0.7933-0.7934) than did the Fine and Gray model (C-index: 0.7550, 0.7510-0.7583). The three-dimensional cumulative incidence curves derived from nonlinear model were used to identify the change points of the risk trends. It would be useful to implement these findings in treatment plans and follow-up surveillance in nonmetastatic CRC patients.
Keywords: time-dependent effects; Colorectal cancer; SEER; nonlinear effects.
© 2017 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Figures
References
-
- Torre, L. A. , Bray F., Siegel R. L., Ferlay J., Lortet‐Tieulent J., and Jemal A.. 2015. Global cancer statistics, 2012. CA Cancer J. Clin. 65:87–108. - PubMed
-
- Siegel, R. L. , Miller K. D., and Jemal A.. 2015. Cancer statistics, 2015. CA Cancer J. Clin. 65:5–29. - PubMed
-
- Zheng, R. , Zeng H., Zhang S., Chen T., and Chen W.. 2016. National estimates of cancer prevalence in China, 2011. Cancer Lett. 370:33–38. - PubMed
-
- Kim, M. J. , Jeong S. Y., Choi S. J., Ryoo S. B., J. W. Park , Park K. J., et al. 2015. Survival paradox between stage IIB/C (T4N0) and stage IIIA (T1‐2N1) colon cancer. Ann. Surg. Oncol. 22:505–512. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
