

Geographical assignment of hospitalists in an urban teaching hospital: feasibility and impact on efficiency and provider satisfaction
- PMID: 28707548
- PMCID: PMC6954492
- DOI: 10.1080/21548331.2017.1353884
Geographical assignment of hospitalists in an urban teaching hospital: feasibility and impact on efficiency and provider satisfaction
Abstract
Objective: To evaluate whether implementation of a geographic model of assigning hospitalists is feasible and sustainable in a large hospitalist program and assess its impact on provider satisfaction, perceived efficiency and patient outcomes.
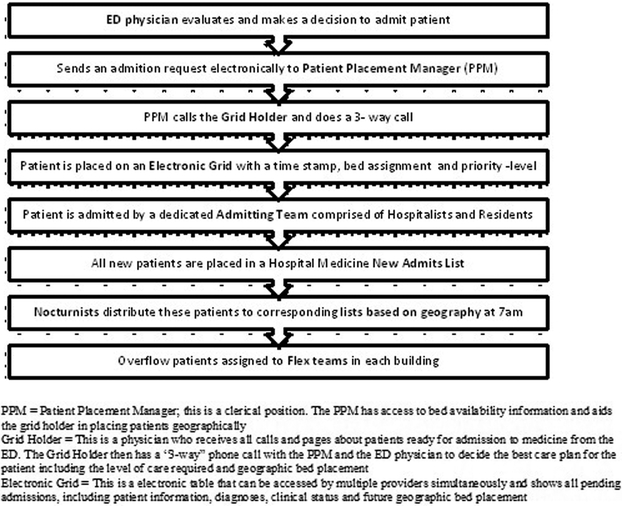
Methods: Pre (3 months) - post (12 months) intervention study conducted from June 2014 through September 2015 at a tertiary care medical center with a large hospitalist program caring for patients scattered in 4 buildings and 16 floors. Hospitalists were assigned to a particular nursing unit (geographic assignment) with a goal of having over 80% of their assigned patients located on their assigned unit. Satisfaction and perceived efficiency were assessed through a survey administered before and after the intervention.
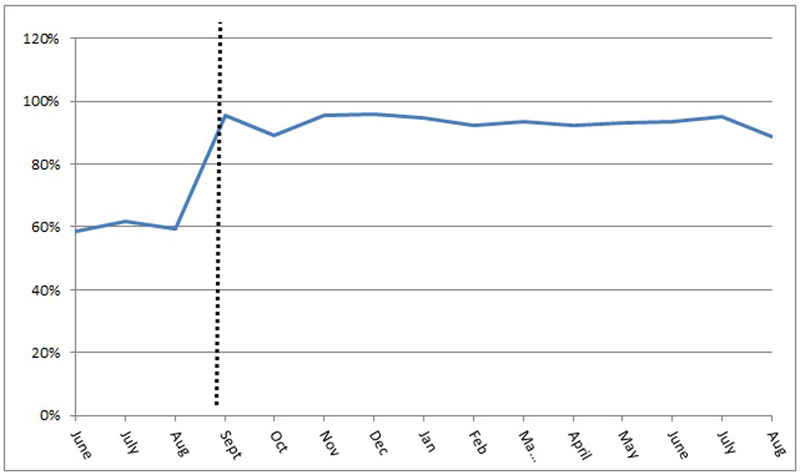
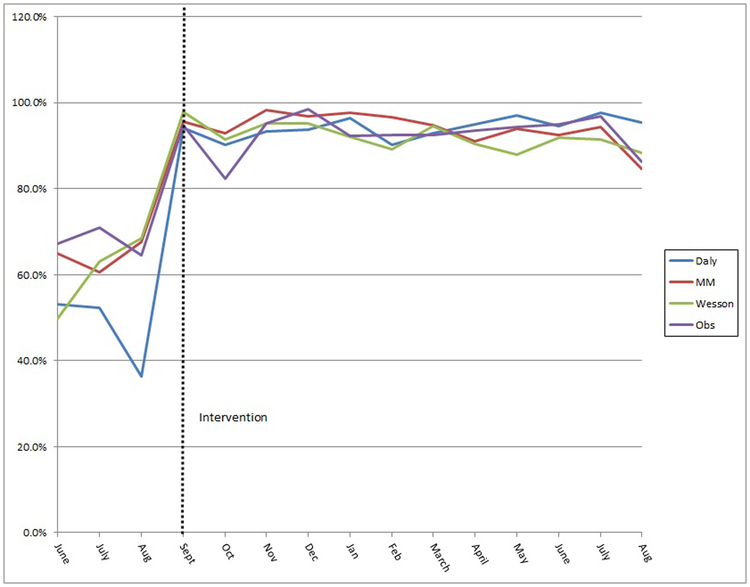
Results: Geographic assignment percentage increased from an average of 60% in the pre-intervention period to 93% post-intervention. The number of hospitalists covering a 32 bed unit decreased from 8-10 pre to 2-3 post-intervention. A majority of physicians (87%) thought that geography had a positive impact on the overall quality of care. Respondents reported that they felt that geography increased time spent with patient/caregivers to discuss plan of care (p < 0.001); improved communication with nurses (p = 0.0009); and increased sense of teamwork with nurses/case managers (p < 0.001). Mean length of stay (4.54 vs 4.62 days), 30-day readmission rates (16.0% vs 16.6%) and patient satisfaction (79.9 vs 77.3) did not change significantly between the pre- and post-implementation period. The discharge before noon rate improved slightly (47.5% - 54.1%).
Conclusions: Implementation of a unit-based model in a large hospitalist program is feasible and sustainable with appropriate planning and support. The geographical model of care increased provider satisfaction and perceived efficiency; it also facilitated the implementation of other key interventions such as interdisciplinary rounds.
Keywords: Geographic assignment; hospitalist deployment; provider satisfaction with rounding; unit based rounding.
Conflict of interest statement
Declaration of Interests
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Figures
Comment in
-
Wide-reaching effects of and concerns regarding geographic localization of hospitalist units.Hosp Pract (1995). 2018 Feb;46(1):43-44. doi: 10.1080/21548331.2018.1406775. Epub 2017 Nov 22. Hosp Pract (1995). 2018. PMID: 29141470 No abstract available.
-
Authors reply: wide-reaching effects of and concerns regarding geographic localization of hospitalist units.Hosp Pract (1995). 2018 Feb;46(1):45. doi: 10.1080/21548331.2018.1406776. Epub 2017 Nov 23. Hosp Pract (1995). 2018. PMID: 29157046 No abstract available.
References
-
- Wachter RM, Goldman L. Zero to 50,000 - The 20th Anniversary of the Hospitalist. N Engl J Med. 2016;375(11):1009–1011. - PubMed
-
- Wertheimer B, Jacobs RE, Bailey M, et al. Discharge before noon: an achievable hospital goal. J Hosp Med. 2014;9(4):210–214. - PubMed
-
- Starmer AJ, Spector ND, Srivastava R, et al. Changes in medical errors after implementation of a handoff program. N Engl J Med. 2014;371(19):1803–1812. - PubMed
-
- O’Leary KJ, Haviley C, Slade ME, Shah HM, Lee J, Williams MV. Improving teamwork: impact of structured interdisciplinary rounds on a hospitalist unit. J Hosp Med. 2011;6(2):88–93. - PubMed
-
- Artenstein AW, Higgins TL, Seiler A, et al. Promoting high value inpatient care via a coaching model of structured, interdisciplinary team rounds. Br J Hosp Med (Lond). 2015;76(1):41–45. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources