

Relationship between Race and the Effect of Fluids on Long-term Mortality after Acute Respiratory Distress Syndrome. Secondary Analysis of the National Heart, Lung, and Blood Institute Fluid and Catheter Treatment Trial
- PMID: 28708421
- PMCID: PMC5711400
- DOI: 10.1513/AnnalsATS.201611-906OC
Relationship between Race and the Effect of Fluids on Long-term Mortality after Acute Respiratory Distress Syndrome. Secondary Analysis of the National Heart, Lung, and Blood Institute Fluid and Catheter Treatment Trial
Abstract
Rationale: Short-term follow-up in the Fluid and Catheter Treatment Trial (FACTT) suggested differential mortality by race with conservative fluid management, but no significant interaction.
Objective: In a post hoc analysis of FACTT including 1-year follow-up, we sought to estimate long-term mortality by race and test for an interaction between fluids and race.
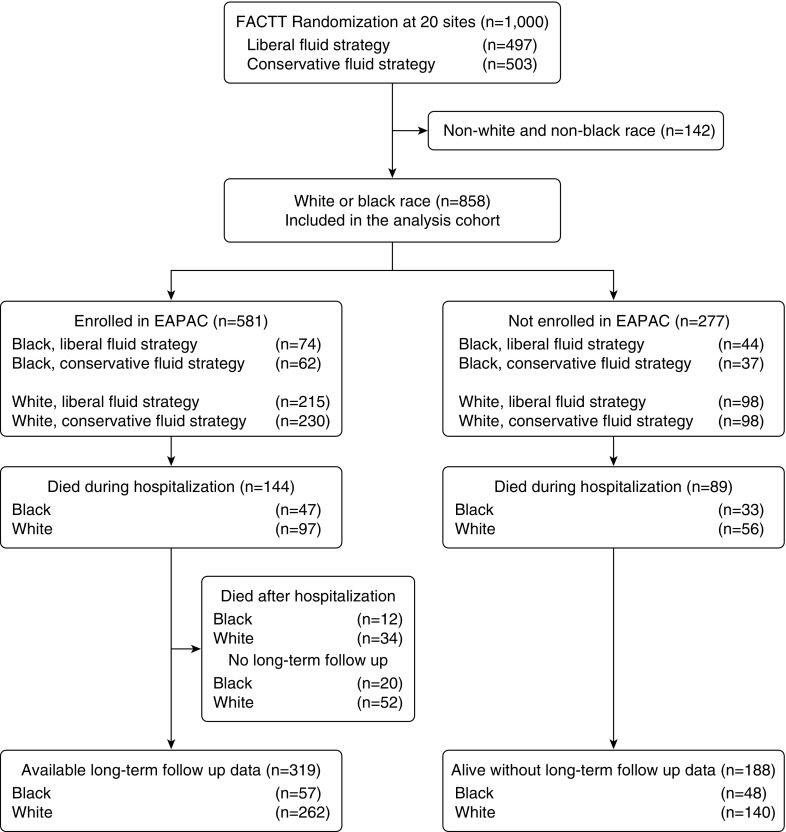
Methods: We performed a post hoc analysis of FACTT and the Economic Analysis of Pulmonary Artery Catheters (EAPAC) study (which included 655 of the 1,000 FACTT patients with near-complete 1-year follow up). We fit a multistate Markov model to estimate 1-year mortality for all non-Hispanic black and white randomized FACTT subjects. The model estimated the distribution of time from randomization to hospital discharge or hospital death (available on all patients) and estimated the distribution of time from hospital discharge to death using data on patients after hospital discharge for patients in EAPAC. The 1-year mortality was found by combining these estimates.
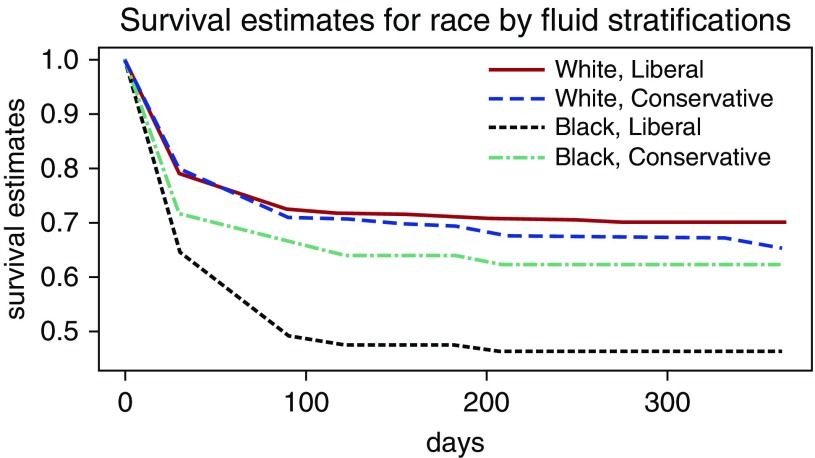
Results: Non-Hispanic black (n = 217, 25%) or white identified subjects (n = 641, 75%) were included. There was a significant interaction between race and fluid treatment (P = 0.012). One-year mortality was lower for black subjects assigned to conservative fluids (38 vs. 54%; mean mortality difference, 16%; 95% confidence interval, 2-30%; P = 0.027 between conservative and liberal). Conversely, 1-year mortality for white subjects was 35% versus 30% for conservative versus liberal arms (mean mortality difference, -4.8%; 95% confidence interval, -13% to 3%; P = 0.23).
Conclusions: In our cohort, conservative fluid management may have improved 1-year mortality for non-Hispanic black patients with ARDS. However, we found no long-term benefit of conservative fluid management in white subjects.
Figures
Comment in
-
Fluid Management in Acute Respiratory Distress Syndrome: Do We Have All the FACTTs to Determine the Effect of Race?Ann Am Thorac Soc. 2017 Sep;14(9):1391-1392. doi: 10.1513/AnnalsATS.201706-501ED. Ann Am Thorac Soc. 2017. PMID: 28862495 Free PMC article. No abstract available.
References
-
- Wiedemann HP, Wheeler AP, Bernard GR, Thompson BT, Hayden D, deBoisblanc B, Connors AF, Jr, Hite RD, Harabin AL National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006;354:2564–2575. - PubMed
-
- Rivers EP. Fluid-management strategies in acute lung injury: liberal, conservative, or both? N Engl J Med. 2006;354:2598–2600. - PubMed
-
- Schuller D, Mitchell JP, Calandrino FS, Schuster DP. Fluid balance during pulmonary edema: is fluid gain a marker or a cause of poor outcome? Chest. 1991;100:1068–1075. - PubMed
-
- Schuster DP. The case for and against fluid restriction and occlusion pressure reduction in adult respiratory distress syndrome. New Horiz. 1993;1:478–488. - PubMed
-
- Maitland K, Kiguli S, Opoka RO, Engoru C, Olupot-Olupot P, Akech SO, Nyeko R, Mtove G, Reyburn H, Lang T, et al. FEAST Trial Group. Mortality after fluid bolus in African children with severe infection. N Engl J Med. 2011;364:2483–2495. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
