

Mortality outcomes of low-dose computed tomography screening for lung cancer in urban China: a decision analysis and implications for practice
- PMID: 28709441
- PMCID: PMC5512753
- DOI: 10.1186/s40880-017-0221-8
Mortality outcomes of low-dose computed tomography screening for lung cancer in urban China: a decision analysis and implications for practice
Abstract
Background: Mortality outcomes in trials of low-dose computed tomography (CT) screening for lung cancer are inconsistent. This study aimed to evaluate whether CT screening in urban areas of China could reduce lung cancer mortality and to investigate the factors that associate with the screening effect.
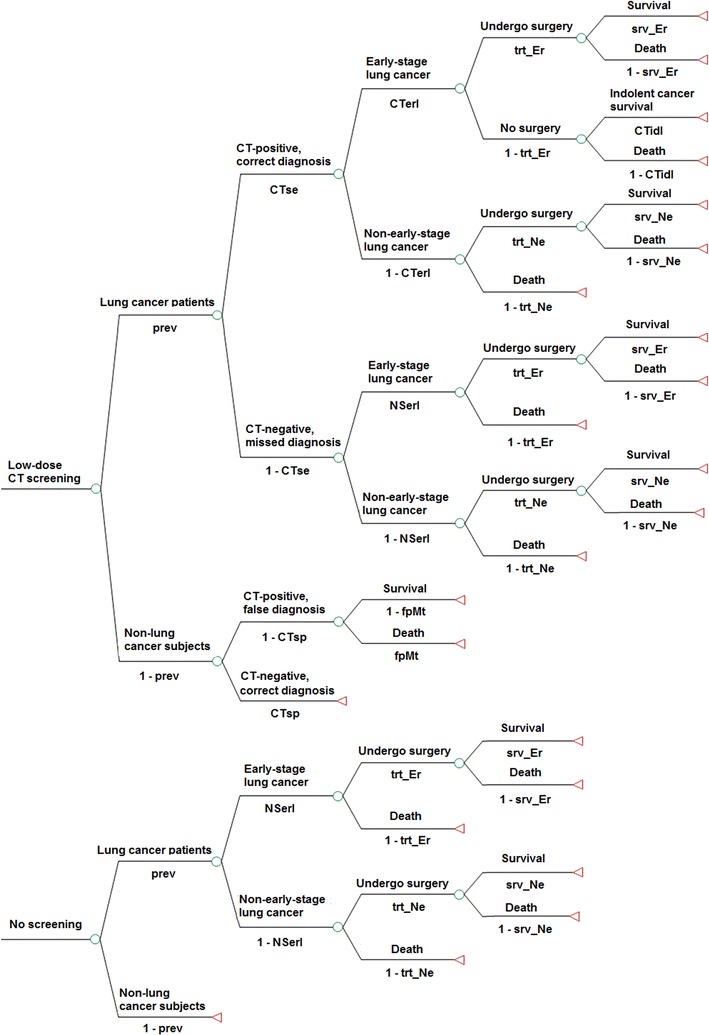
Methods: A decision tree model with three scenarios (low-dose CT screening, chest X-ray screening, and no screening) was developed to compare screening results in a simulated Chinese urban cohort (100,000 smokers aged 45-80 years). Data of participant characteristics were obtained from national registries and epidemiological surveys for estimating lung cancer prevalence. The selection of other tree variables such as sensitivities and specificities of low-dose CT and chest X-ray screening were based on literature research. Differences in lung cancer mortality (primary outcome), false diagnoses, and deaths due to false diagnosis were calculated. Sensitivity analyses were performed to identify the factors that associate with the screening results and to ascertain worst and optimal screening effects considering possible ranges of the variables.
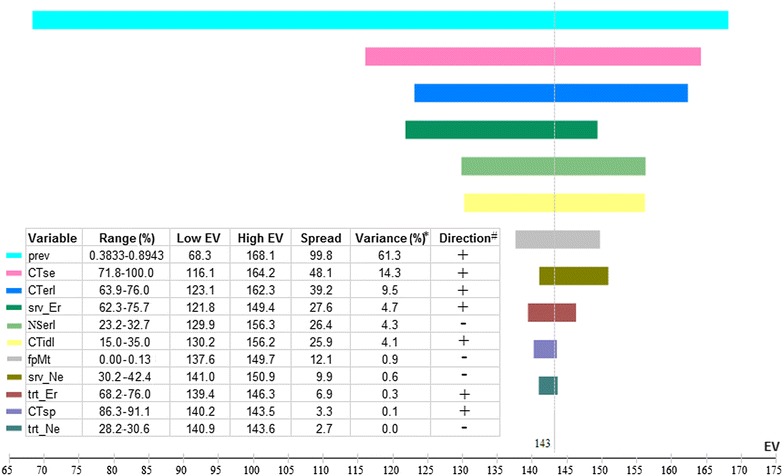
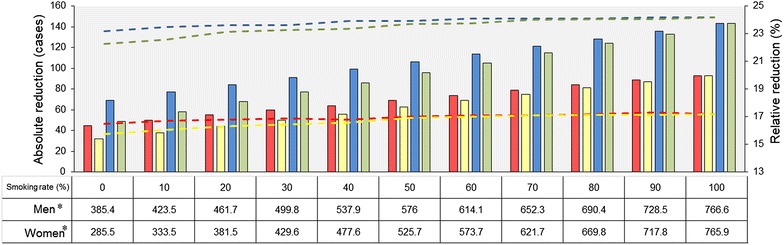
Results: Among the 100,000 subjects, there were 448, 541, and 591 lung cancer deaths in the low-dose CT, chest X-ray, and no screening scenarios, respectively (17.2% reduction in low-dose CT screening over chest X-ray screening and 24.2% over no screening). The costs of the two screening scenarios were 9387 and 2497 false diagnoses and 7 and 2 deaths due to false diagnosis among the 100,000 persons, respectively. The factors that most influenced death reduction with low-dose CT screening over no screening were lung cancer prevalence in the screened cohort, low-dose CT sensitivity, and proportion of early-stage cancers among low-dose CT detected lung cancers. Considering all possibilities, reduction in deaths (relative numbers) with low-dose CT screening in the worst and optimal cases were 16 (5.4%) and 288 (40.2%) over no screening, respectively.
Conclusions: In terms of mortality outcomes, our findings favor conducting low-dose CT screening in urban China. However, approaches to reducing false diagnoses and optimizing important screening conditions such as enrollment criteria for screening are highly needed.
Keywords: Decision analysis; Low-dose CT; Lung cancer; Mortality outcome; Screening.
Figures
References
-
- American Cancer Society. Cancer facts & figures 2014. http://www.cancer.org/research/cancerfactsstatistics/cancerfactsfigures2.... Accessed 28 Aug 2016.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
