

Severity of acute gastrointestinal injury grade is a predictor of all-cause mortality in critically ill patients: a multicenter, prospective, observational study
- PMID: 28709443
- PMCID: PMC5513140
- DOI: 10.1186/s13054-017-1780-4
Severity of acute gastrointestinal injury grade is a predictor of all-cause mortality in critically ill patients: a multicenter, prospective, observational study
Abstract
Background: In 2012, the European Society of Intensive Care Medicine proposed a definition for acute gastrointestinal injury (AGI) based on current medical evidence and expert opinion. The aim of the present study was to evaluate the feasibility of using the current AGI grading system and to investigate the association between AGI severity grades with clinical outcome in critically ill patients.
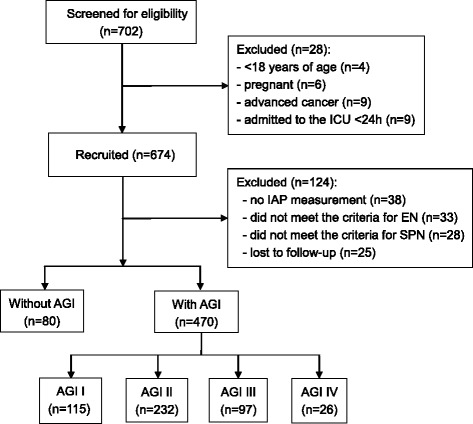
Methods: Adult patients at 14 general intensive care units (ICUs) with an expected ICU stay ≥24 h were prospectively studied. The AGI grade was assessed daily on the basis of gastrointestinal (GI) symptoms, intra-abdominal pressures, and feeding intolerance (FI) in the first week of admission to the ICU.
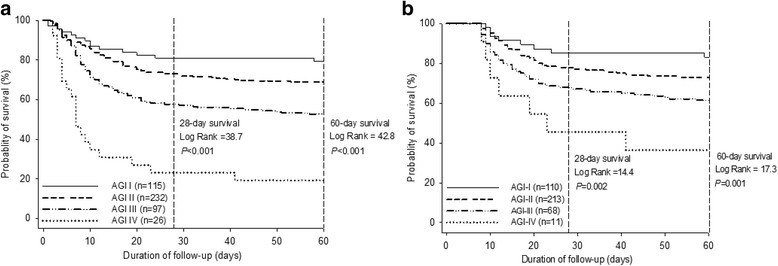
Results: Among the 550 patients enrolled, 456 patients (82.9%) received mechanical ventilation, and 470 patients were identified for AGI. The distribution of the global AGI grade was 24.5% with grade I, 49.4% with grade II, 20.6% with grade III, and 5.5% with grade IV. AGI grading was positively correlated with 28- and 60-day mortality (P < 0.0001). Univariate Cox regression analysis showed that age, sepsis, diabetes mellitus, coronary artery disease, the use of vasoactive drugs, serum creatinine and lactate levels, mechanical ventilation, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, and the global AGI grade were significantly (P ≤ 0.02) associated with 60-day mortality. In a multivariate analysis including these variables, diabetes mellitus (HR 1.43, 95% CI 1.03-1.87; P = 0.05), the use of vasoactive drugs (HR 1.56, 95% CI 1.12-2.11; P = 0.01), serum lactate (HR 1.15, 95% CI 1.06-1.24; P = 0.03), global AGI grade (HR 1.65, 95% CI 1.28-2.12; P = 0.008), and APACHE II score (HR 1.04, 95% CI 1.02-1.06; P < 0.001) were independently associated with 60-day mortality. In a subgroup analysis of 402 patients with 7-day survival, in addition to clinical predictors and the AGI grade on the first day of ICU stay, FI within the first week of ICU stay had an independent and incremental prognostic value for 60-day mortality (χ2 = 41.9 vs. 52.2, P = 0.007).
Conclusions: The AGI grading scheme is useful for identifying the severity of GI dysfunction and could be used as a predictor of impaired outcomes. In addition, these results support the hypothesis that persistent FI within the first week of ICU stay is an independent determinant for mortality.
Trial registration: Chinese Clinical Trial Registry identifier: ChiCTR-OCS-13003824 . Registered on 29 September 2013.
Keywords: Acute gastrointestinal injury; Critically ill patients; Feeding intolerance; Mortality.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was approved by the local ethics committee for each hospital (Zhejiang Provincial People’s Hospital, Sir Run Run Shaw Hospital Zhejiang University School of Medicine, Shaoxing People’s Hospital, Jinhua People’s Hospital, The Third Affiliated Hospital of Zhejiang Chinese Medical University, The First Hospital of Jiaxing, Hangzhou First People’s Hospital, Ningbo Medical Treatment Center Lihuili Hospital, The First Affiliated Hospital of Zhejiang Chinese Medical University, The Second Affiliated Hospital of Zhejiang Chinese Medical University, Taizhou Hospital of Zhejiang Province, Zhuji People’s Hospital of Zhejiang Province, the Central Hospital of Lishui City, Huzhou Central Hospital). All patients or their legal representatives provided informed written consent according to the local ethics rules.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Reintam Blaser A, Malbrain ML, Starkopf J, Fruhwald S, Jakob SM, De Waele J, et al. Gastrointestinal function in intensive care patients: terminology, definitions and management. Recommendations of the ESICM Working Group on Abdominal Problems. Intensive Care Med. 2012;38(3):384–394. doi: 10.1007/s00134-011-2459-y. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
