

Barriers and facilitators to reducing frequent laboratory testing for patients who are stable on warfarin: a mixed methods study of de-implementation in five anticoagulation clinics
- PMID: 28709455
- PMCID: PMC5513354
- DOI: 10.1186/s13012-017-0620-x
Barriers and facilitators to reducing frequent laboratory testing for patients who are stable on warfarin: a mixed methods study of de-implementation in five anticoagulation clinics
Abstract
Background: Patients on chronic warfarin therapy require regular laboratory monitoring to safely manage warfarin. Recent studies have challenged the need for routine monthly blood draws in the most stable warfarin-treated patients, suggesting the safety of less frequent laboratory testing (up to every 12 weeks). De-implementation efforts aim to reduce the use of low-value clinical practices. To explore barriers and facilitators of a de-implementation effort to reduce the use of frequent laboratory tests for patients with stable warfarin management in nurse/pharmacist-run anticoagulation clinics, we performed a mixed-methods study conducted within a state-wide collaborative quality improvement collaborative.
Methods: Using a mixed-methods approach, we conducted post-implementation semi-structured interviews with a total of eight anticoagulation nurse or pharmacist staff members at five participating clinic sites to assess barriers and facilitators to de-implementing frequent international normalized ratio (INR) laboratory testing among patients with stable warfarin control. Interview guides were based on the Tailored Implementation for Chronic Disease (TICD) framework. Informed by interview themes, a survey was developed and administered to all anticoagulation clinical staff (n = 62) about their self-reported utilization of less frequent INR testing and specific barriers to de-implementing the standard (more frequent) INR testing practice.
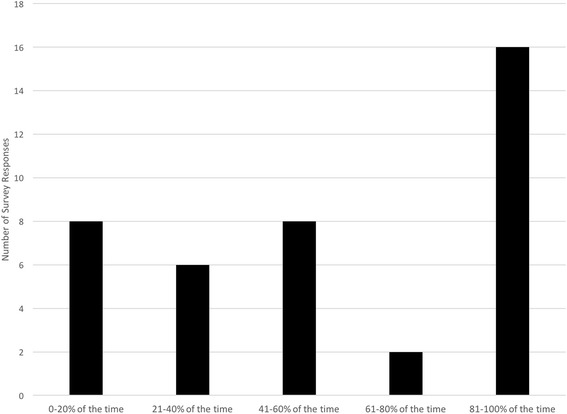
Results: From the interviews, four themes emerged congruent with TICD domains: (1) staff overestimating their actual use of less frequent INR testing (individual health professional factors), (2) barriers to appropriate patient engagement (incentives and resources), (3) broad support for an electronic medical record flag to identify potentially eligible patients (incentives and resources), and (4) the importance of personalized nurse/pharmacist feedback (individual health professional factors). In the survey (65% response rate), staff report offering less frequent INR testing to 56% (46-66%) of eligible patients. Most survey responders (n = 24; 60%) agreed that an eligibility flag in the electronic medical record would be very helpful. Twenty-four (60%) respondents agreed that periodic, personalized feedback on use of less frequent INR testing would also be helpful.
Conclusions: Leveraging information system notifications, reducing additional work load burden for participating patients and providers, and providing personalized feedback are strategies that may improve adoption and utilization new policies in anticoagulation clinics that focus on de-implementation.
Keywords: Anticoagulation; Implementation; Quality improvement; Warfarin.
Conflict of interest statement
Ethics approval and consent to participate
This study was reviewed by the University of Michigan Institutional Review Board and deemed not regulated as a quality improvement project.
Consent for publication
Not applicable.
Competing interests
GB reports research grant funding from Blue Cross-Blue Shield of Michigan and Pfizer/BMS. He reports consulting fees from Aralez and Pfizer/BMS.
SM reports no competing interests
SK reports speaker honorarium from Janssen, Boehringer-Ingelheim, Bristol Myer Squibb, Pfizer, CSL Behring, Daiichi Sankyo; consultant fees from Boehringer Ingelheim, Bristol Myer Squibb, Pfizer, Janssen
Daiichi Sankyo, Portola. Research funding (to institution): Janssen
LAJ reports no competing interests
BH reports no competing interests
EKR reports consulting fees from Janssen and board membership in the Anticoagulation Forum
JK reports no competing interests
GK reports no competing interests
JBF Consultant: Boehringer Ingelheim, Bristol Myer Squibb, Pfizer, Janssen, Merck. Research Funding: Janssen, Pfizer, Blue Cross-Blue Shield of Michigan
AS reports serving and co-editor-in-chief for Implementation Science
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Schulman S, Parpia S, Stewart C, Rudd-Scott L, Julian JA, Levine M. Warfarin dose assessment every 4 weeks versus every 12 weeks in patients with stable international normalized ratios: a randomized trial. Ann Intern Med. 2011;155:653–659. doi: 10.7326/0003-4819-155-10-201111150-00003. - DOI - PubMed
-
- Rose AJ, Ozonoff A, Berlowitz DR, Ash AS, Reisman JI, Hylek EM. Reexamining the recommended follow-up interval after obtaining an in-range international normalized ratio value: results from the Veterans Affairs study to improve anticoagulation. Chest. 2011;140:359–365. doi: 10.1378/chest.10-2738. - DOI - PubMed
-
- Holbrook A, Schulman S, Witt DM, Vandvik PO, Fish J, Kovacs MJ, Svensson PJ, Veenstra DL, Crowther M, Guyatt GH, American College of Chest P Evidence-based management of anticoagulant therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141:e152S–e184S. doi: 10.1378/chest.11-2295. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
