

The Clinical and Economic Effect of Vascular Access Selection in Patients Initiating Hemodialysis with a Catheter
- PMID: 28710090
- PMCID: PMC5698057
- DOI: 10.1681/ASN.2016060707
The Clinical and Economic Effect of Vascular Access Selection in Patients Initiating Hemodialysis with a Catheter
Abstract
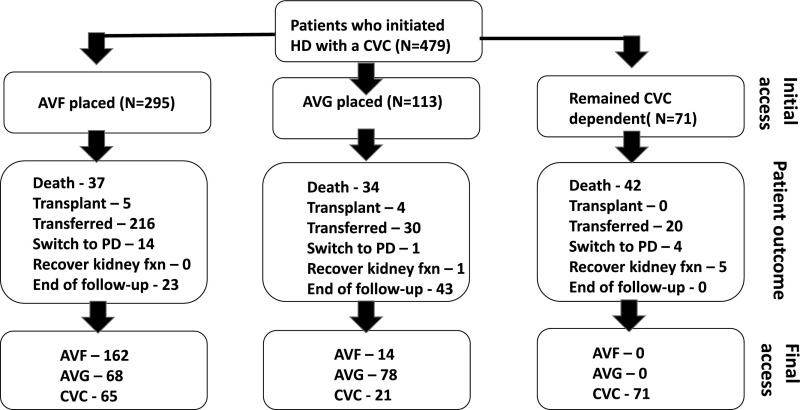
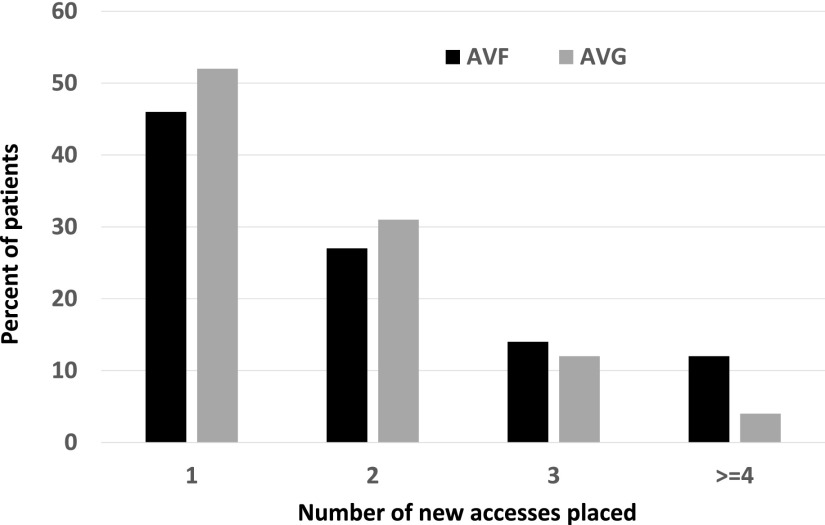
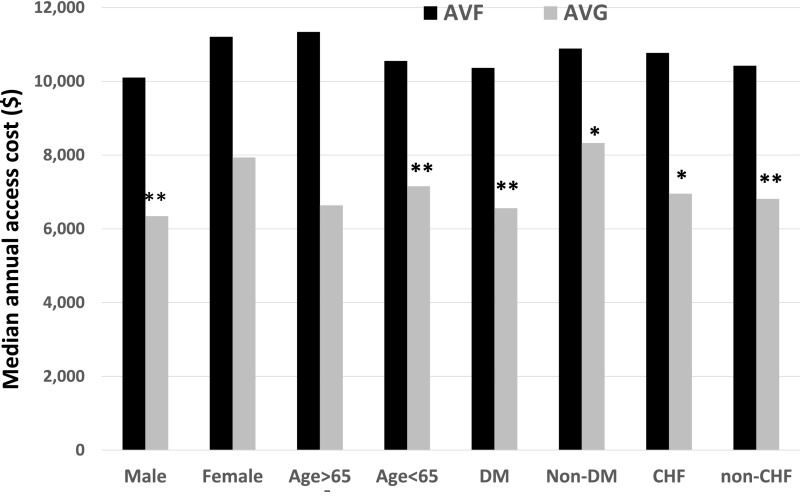
Patients in the United States frequently initiate hemodialysis with a central venous catheter (CVC) and subsequently undergo placement of a new arteriovenous fistula (AVF) or arteriovenous graft (AVG). Little is known about the clinical and economic effects of initial vascular access choice. We identified 479 patients starting hemodialysis with a CVC at a large medical center (during 2004-2012) who subsequently had an AVF (n=295) or AVG (n=105) placed or no arteriovenous access (CVC group, n=71). Compared with patients receiving an AVG, those receiving an AVF had more frequent surgical access procedures per year (1.01 [95% confidence interval, 0.95 to 1.08] versus 0.62 [95% confidence interval, 0.55 to 0.70]; P<0.001) but a similar frequency of percutaneous access procedures per year. Patients receiving an AVF had a higher median annual cost (interquartile range) of surgical access procedures than those receiving an AVG ($4857 [$2523-$8835] versus $2819 [$1411-$4274]; P<0.001), whereas the annual cost of percutaneous access procedures was similar in both groups. The AVF group had a higher median overall annual access-related cost than the AVG group ($10,642 [$5406-$19,878] versus $6810 [$3718-$13,651]; P=0.001) after controlling for patient age, sex, race, and diabetes. The CVC group had the highest median annual overall access-related cost ($28,709 [$11,793-$66,917]; P<0.001), largely attributable to the high frequency of hospitalizations due to catheter-related bacteremia. In conclusion, among patients initiating hemodialysis with a CVC, the annual cost of access-related procedures and complications is higher in patients who initially receive an AVF versus an AVG.
Keywords: arteriovenous access; arteriovenous fistula; arteriovenous graft.
Copyright © 2017 by the American Society of Nephrology.
Figures
References
-
- KDOQI clinical practice guidelines and clinical practice recommendations for vascular access 2006. Am J Kidney Dis 48[Suppl 1]: S176–S322, 2006 - PubMed
-
- Allon M: Current management of vascular access. Clin J Am Soc Nephrol 2: 786–800, 2007 - PubMed
-
- Collins AJ, Foley RN, Gilbertson DT, Chen SC: The state of chronic kidney disease, ESRD, and morbidity and mortality in the first year of dialysis. Clin J Am Soc Nephrol 4[Suppl 1]: S5–S11, 2009 - PubMed
-
- Xue JL, Dahl D, Ebben JP, Collins AJ: The association of initial hemodialysis access type with mortality outcomes in elderly Medicare ESRD patients. Am J Kidney Dis 42: 1013–1019, 2003 - PubMed
-
- Allon M, Dinwiddie L, Lacson E Jr, Latos DL, Lok CE, Steinman T, Weiner DE: Medicare reimbursement policies and hemodialysis vascular access outcomes: A need for change. J Am Soc Nephrol 22: 426–430, 2011 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
