

Xpert HIV-1 point-of-care test for neonatal diagnosis of HIV in the birth testing programme of a maternity hospital: a field evaluation study
- PMID: 28711526
- PMCID: PMC5623143
- DOI: 10.1016/S2352-3018(17)30097-8
Xpert HIV-1 point-of-care test for neonatal diagnosis of HIV in the birth testing programme of a maternity hospital: a field evaluation study
Abstract
Background: Point-of-care testing (POCT) among HIV-exposed infants might improve linkage to care relative to laboratory-based testing (LABT). We evaluated HIV-1 POCT at birth in the context of universal LABT in a maternity hospital and describe our implementation experience.
Methods: We did a field evaluation study between Oct 1, 2014, and April 30, 2016, at the urban Rahima Moosa Mother and Child Hospital (RMMCH), Johannesburg, South Africa. We aimed to sample consecutive neonates at birth with POCT (Cepheid Xpert HIV-1 Qualitative test) and compared results with those of LABT (Roche COBAS TaqMan HIV-1 Qualitative test) with respect to performance in terms of sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and Cohen's κ coefficient, result return, antiretroviral treatment (ART) initiation, and coverage.
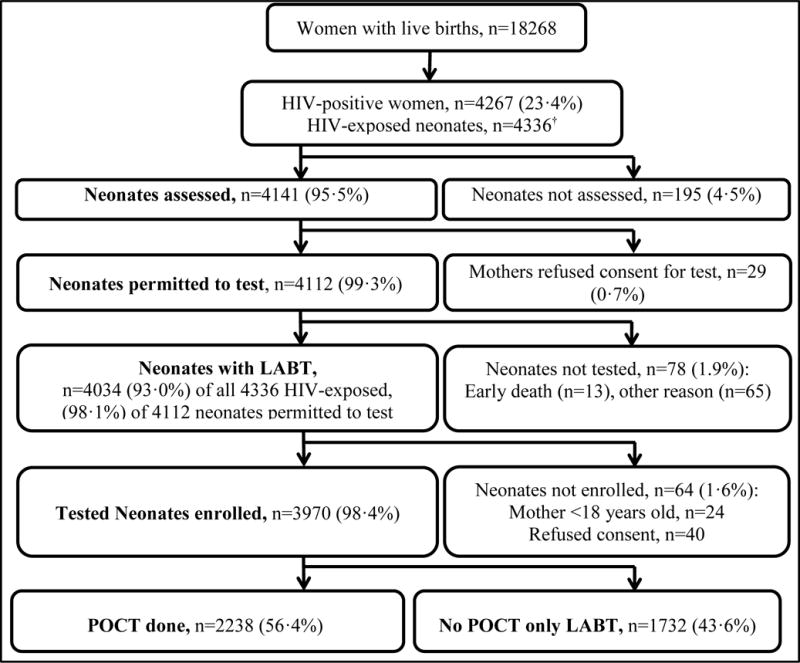
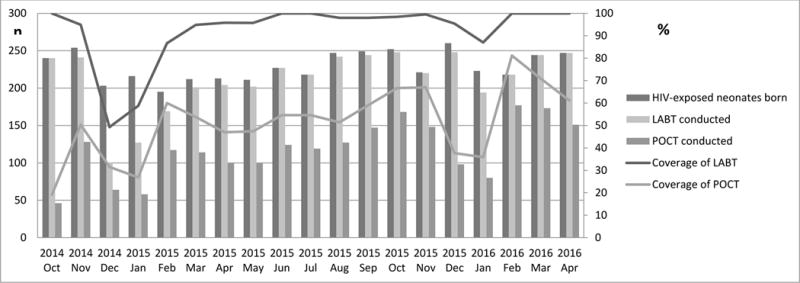
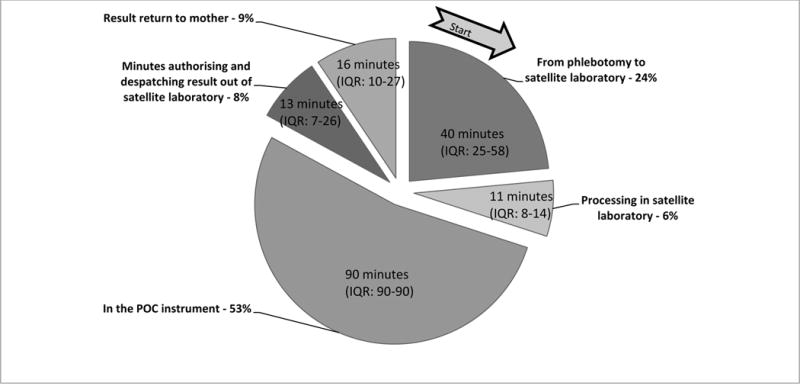
Findings: 18 268 women delivered livebirths at RMMCH and 4267 (23%) were HIV-positive with 4336 HIV-exposed neonates delivered. Mothers of 4141 (96%) HIV-exposed neonates were offered infant birth testing. Mothers of 4112 (99%) neonates consented. In 78 neonates with consent (2%), a test was not done due to early neonatal death (n=13), mother departing before venesection, or staff unavailability. Among 3970 infants who had LABT, 57 (1%) tested positive, 3906 (99%) tested negative, two (<1%) were indeterminate, and five (<1%) had an error result. 2238 (56%) of these infants had concurrent POCT. POCT detected all 30 HIV-infected neonates (sensitivity 100%; 95% CI 88·4-100) with two additional false-positive results (specificity 99·9%; 99·7-100). All positive and 96·2% of negative POCT results were returned compared with 88·9% of positive and 52·8% of negative LABT results. Although every POCT required 90 min of instrument time, 2·6 h (IQR 2·3-3·1) elapsed between phlebotomy and result return. In days, median time of result return for POCT was 1 day, significantly earlier than 10 days for LABT (p<0·0001). ART was initiated in 30 neonates (100%) with positive POCT compared with 24 (88·9%, p=0·10) of 27 infants who had LABT only, with initiation occurring a median of 5 days earlier in the POCT group (p<0·0001). POCT implementation required additional staff and weekend cover.
Interpretation: Compared with LABT, POCT was associated with good performance, improved rates of result return, and reduced time to ART initiation. Resources needed to integrate POCT into a routine birth testing programme require further evaluation.
Funding: National Institutes of Health.
Copyright © 2017 Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Comment in
-
Paediatric HIV: the unfinished business.Lancet HIV. 2017 Oct;4(10):e425-e427. doi: 10.1016/S2352-3018(17)30126-1. Epub 2017 Jul 12. Lancet HIV. 2017. PMID: 28711527 No abstract available.
References
-
- Bourne DE, Thompson M, Brody LL, et al. Emergence of a peak in early infant mortality due to HIV/AIDS in South Africa. AIDS. 2009;23:101–6. - PubMed
-
- National Department of Health. National consolidated guidelines for the prevention of mother-to-child transmission of HIV (PMTCT) and the management of HIV in children, adolescents and adults. 2015. Pretoria: National Department of Health; 2015.
-
- World Health Organization. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection - recommendations for a public health approach. 2nd. Geneva: World Health Organization; 2016. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
