

Cost and contribution margin of transcatheter versus surgical aortic valve replacement
- PMID: 28712581
- PMCID: PMC6528835
- DOI: 10.1016/j.jtcvs.2017.06.020
Cost and contribution margin of transcatheter versus surgical aortic valve replacement
Abstract
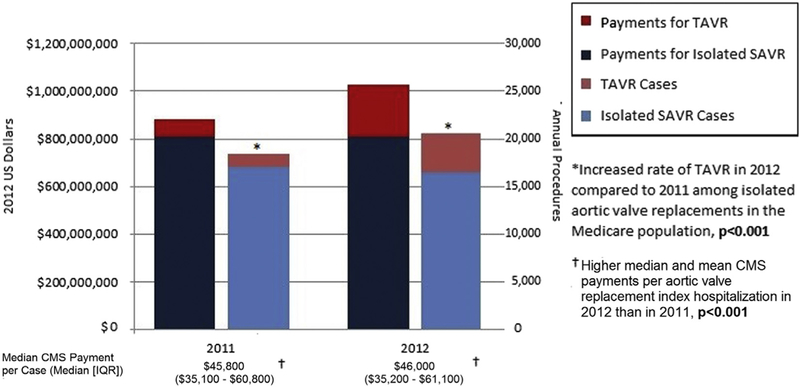
Objective: To compare the cost of and payments for transcatheter aortic valve replacement (TAVR), a novel and expensive technology, and surgical aortic valve replacement (SAVR).
Methods: Medicare claims provided hospital charges, payments, and outcomes between January and December 2012. Hospital costs and charges were estimated using hospital-specific cost-to-charge ratios. Costs and payments were examined in propensity score- matched TAVR and SAVR patients.
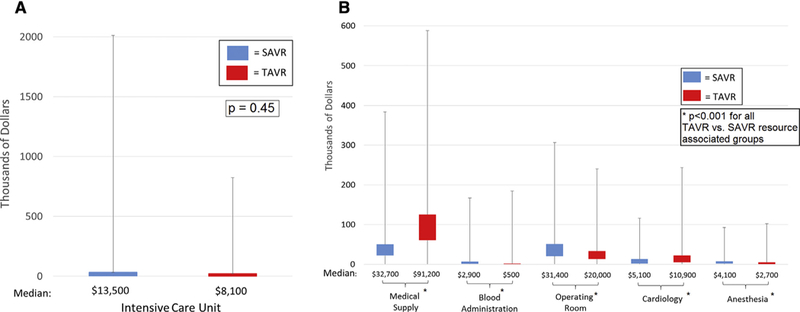
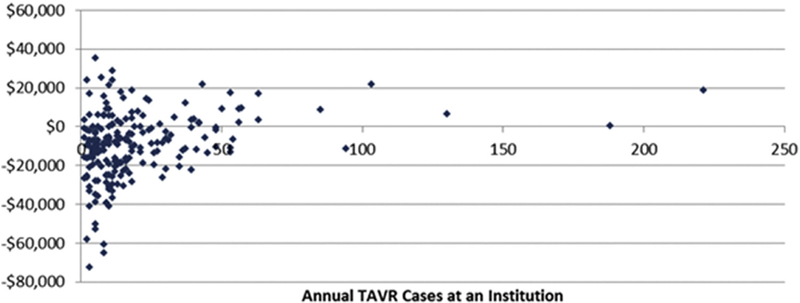
Results: Medicare spent $215,770,200 nationally on 4083 patients who underwent TAVR in 2012. Hospital costs were higher for TAVR patients (median, $50,200; interquartile range [IQR], $39,800-$64,300) than for propensity-matched SAVR patients ($45,500; IQR, $34,500-$63,300; P < .01), owing largely to higher estimated medical supply costs, including the implanted valve prosthesis. Postprocedure hospital length of stay (LOS) length was shorter for TAVR patients (median, 5 days [IQR, 4-8 days] vs 7 days [IQR, 5-9 days]; P < .01), as was total intensive care unit (ICU) LOS (median, 2 days [IQR, 0-5 days] vs 3 days [IQR, 1-6 days]; P < .01). Medicare payments were lower for TAVR hospitalizations (median, $49,500; IQR, $36,900-$64,600) than for SAVR (median, $50,400; IQR, $37,400-$65,800; P < .01). The median of the differences between payments and costs (contribution margin) was -$3380 for TAVR hospitalizations and $2390 for SAVR hospitalizations (P < .01).
Conclusions: TAVR accounted for $215 million in Medicare payments in its first year of clinical use. Among SAVR Medicare patients at a similar risk level, TAVR was associated with higher hospital costs despite shorter ICU LOS and hospital LOS. Overall and/or medical device cost reductions are needed for TAVR to have a net neutral financial impact on hospitals.
Keywords: AVR; SAVR; TAVR; cost.
Copyright © 2017 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest Statement
All other authors have nothing to disclose with regard to commercial support.
Figures
Comment in
-
The costs of operating under a veil of secrecy.J Thorac Cardiovasc Surg. 2017 Dec;154(6):1881-1882. doi: 10.1016/j.jtcvs.2017.08.042. Epub 2017 Aug 30. J Thorac Cardiovasc Surg. 2017. PMID: 28918210 Free PMC article. No abstract available.
-
"Transcatheter aortic valve implantation for everyone": Yes, of course, but how much is that?J Thorac Cardiovasc Surg. 2018 Jun;155(6):2425. doi: 10.1016/j.jtcvs.2018.02.006. J Thorac Cardiovasc Surg. 2018. PMID: 29776288 No abstract available.
-
Providing high-value care at the right price.J Thorac Cardiovasc Surg. 2018 Aug;156(2):606-607. doi: 10.1016/j.jtcvs.2018.01.008. J Thorac Cardiovasc Surg. 2018. PMID: 30011757 No abstract available.
References
-
- Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187–98. - PubMed
-
- Leon MB, Smith CR, Mack MJ, Makkar RR, Svensson LG, Kodali SK, et al. Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. N Engl J Med. 2016;374:1609–20. - PubMed
-
- Leon MB, Smith CR,Mack M, Miller DC,Moses JW, SvenssonL G, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597–607. - PubMed
-
- Mack MJ, Holmes DR Jr. Rational dispersion for the introduction of transcatheter valve therapy. JAMA. 2011;306:2149–50. - PubMed
-
- McCarthy FH, Groeneveld PW, Kobrin D, McDermott KM, Wirtalla C, Desai ND. Effect of clinical trial experience on transcatheter aortic valve replacement outcomes. Circ Cardiovasc Interv. 2015;8:e002234. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
