

Thyroid-Stimulating Hormone Receptor Antibodies in Pregnancy: Clinical Relevance
- PMID: 28713331
- PMCID: PMC5491546
- DOI: 10.3389/fendo.2017.00137
Thyroid-Stimulating Hormone Receptor Antibodies in Pregnancy: Clinical Relevance
Abstract
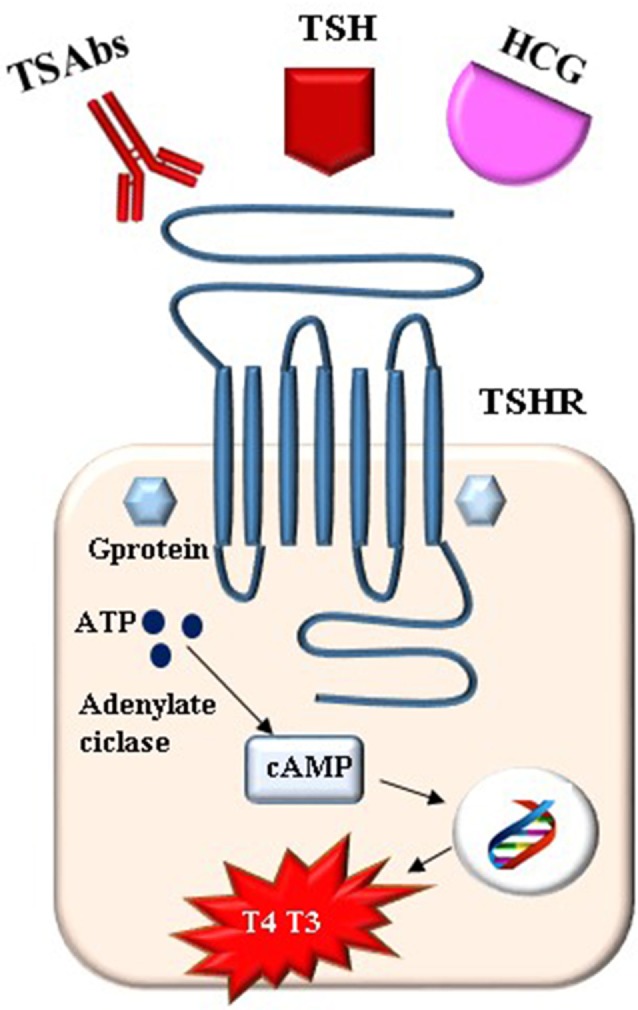
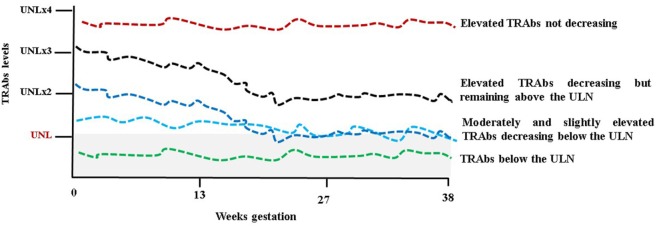
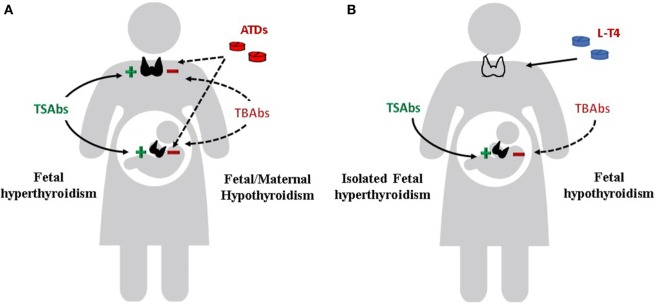
Graves' disease is the most common cause of thyrotoxicosis in women of childbearing age. Approximately 1% of pregnant women been treated before, or are being treated during pregnancy for Graves' hyperthyroidism. In pregnancy, as in not pregnant state, thyroid-stimulating hormone (TSH) receptor (TSHR) antibodies (TRAbs) are the pathogenetic hallmark of Graves' disease. TRAbs are heterogeneous for molecular and functional properties and are subdivided into activating (TSAbs), blocking (TBAbs), or neutral (N-TRAbs) depending on their effect on TSHR. The typical clinical features of Graves' disease (goiter, hyperthyroidism, ophthalmopathy, dermopathy) occur when TSAbs predominate. Graves' disease shows some peculiarities in pregnancy. The TRAbs disturb the maternal as well as the fetal thyroid function given their ability to cross the placental barrier. The pregnancy-related immunosuppression reduces the levels of TRAbs in most cases although they persist in women with active disease as well as in women who received definitive therapy (radioiodine or surgery) before pregnancy. Changes of functional properties from stimulating to blocking the TSHR could occur during gestation. Drug therapy is the treatment of choice for hyperthyroidism during gestation. Antithyroid drugs also cross the placenta and therefore decrease both the maternal and the fetal thyroid hormone production. The management of Graves' disease in pregnancy should be aimed at maintaining euthyroidism in the mother as well as in the fetus. Maternal and fetal thyroid dysfunction (hyperthyroidism as well as hypothyroidism) are in fact associated with several morbidities. Monitoring of the maternal thyroid function, TRAbs measurement, and fetal surveillance are the mainstay for the management of Graves' disease in pregnancy. This review summarizes the biochemical, immunological, and therapeutic aspects of Graves' disease in pregnancy focusing on the role of the TRAbs in maternal and fetal function.
Keywords: Graves’ disease; fetal hyperthyroidism; neonatal hyperthyroidism; pregnancy; thyroid-stimulating hormone receptor antibodies.
Figures
References
-
- Vermiglio F, Moleti M, Trimarchi F. Thyroid diseases in pregnancy. In: Monaco F, editor. Thyroid Diseases. Boca Raton, FL: CRC Press; (2012). p. 425–40.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources