

Overview of robotic thyroidectomy
- PMID: 28713692
- PMCID: PMC5503931
- DOI: 10.21037/gs.2017.03.18
Overview of robotic thyroidectomy
Abstract
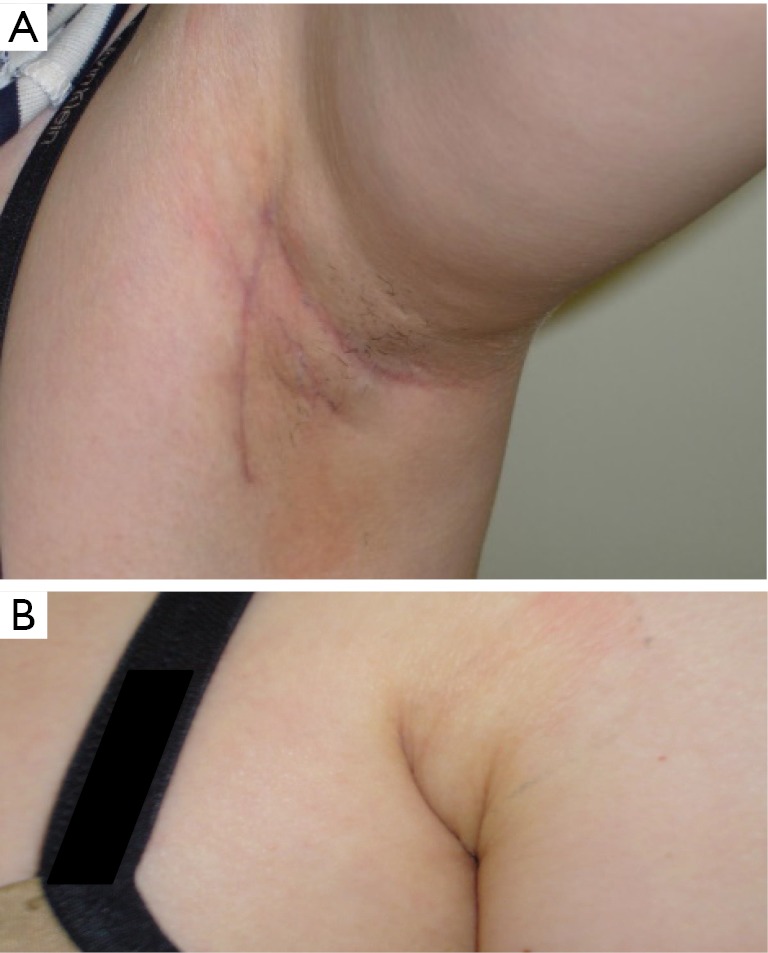
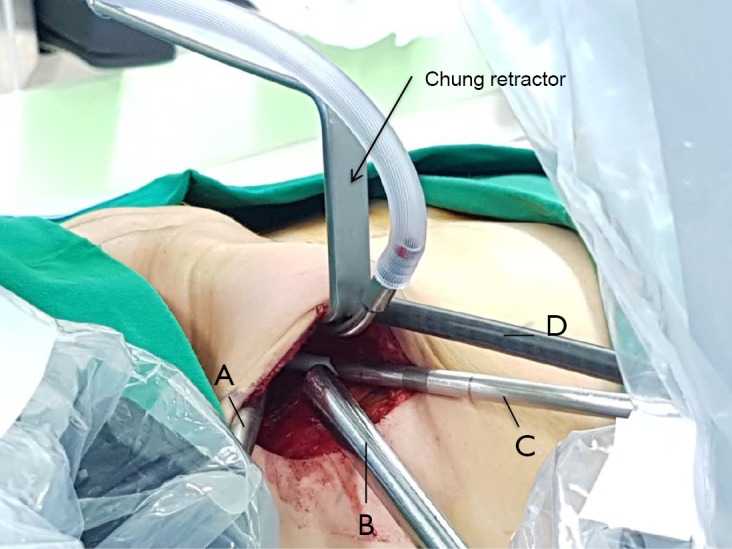
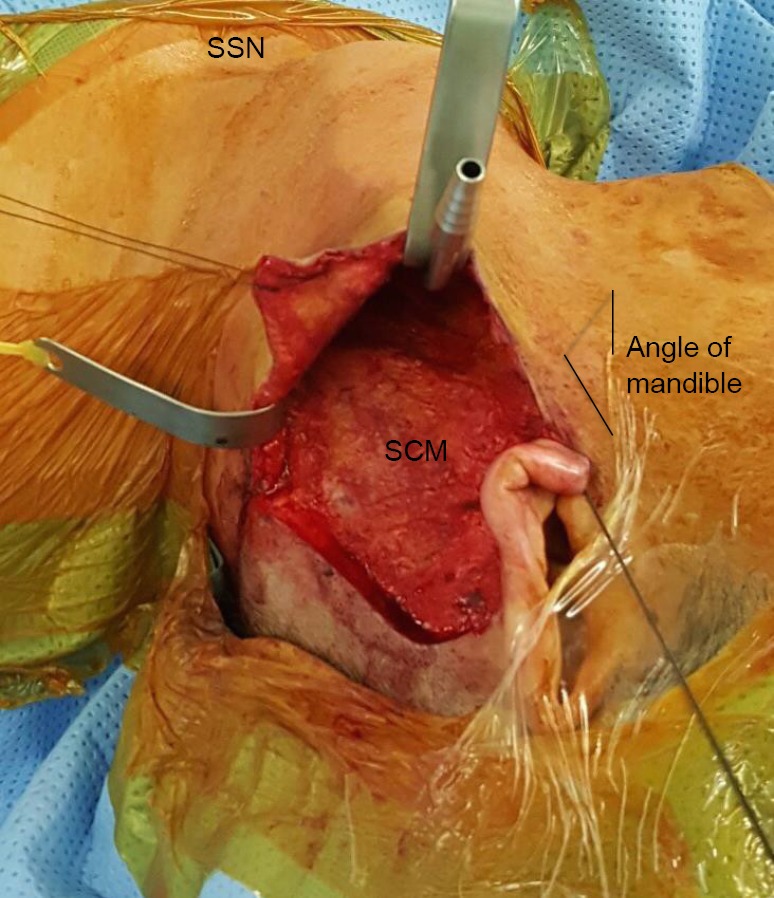
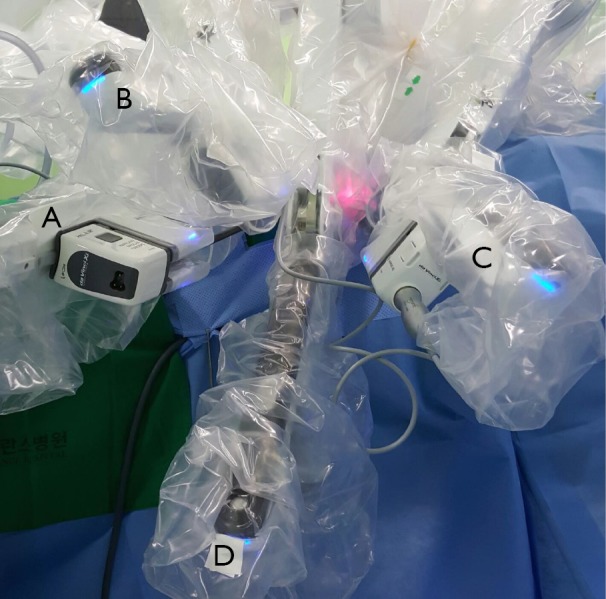
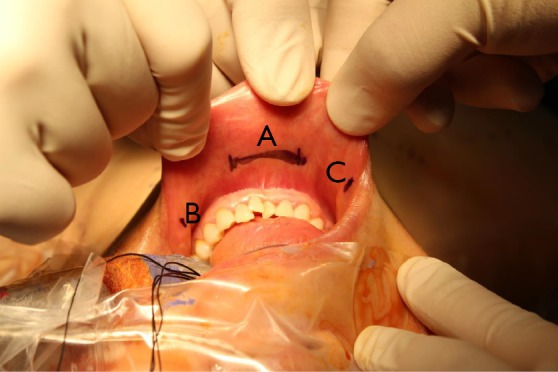
With the advancement and adaptation of technology, there has been a tremendous evolution in the surgical approaches for thyroidectomy. Robotic thyroidectomy has become increasingly popular worldwide attracting both surgeons and patients searching for new and innovative techniques for thyroidectomy with a superior cosmetic result when compared to the conventional open procedures. In this review, we describe the following surgical approaches for robotic thyroidectomy: transaxillary, retroauricular (facelift) and transoral. The advantages and disadvantages as well as limitations of each approach are examined, and future directions of robotic thyroidectomy are discussed.
Keywords: Thyroidectomy; minimally invasive; remote-access; robotic.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources