

Clinical limitations of the International Federation of Gynecology and Obstetrics (FIGO) classification of uterine fibroids
- PMID: 28715088
- PMCID: PMC5629115
- DOI: 10.1002/ijgo.12266
Clinical limitations of the International Federation of Gynecology and Obstetrics (FIGO) classification of uterine fibroids
Abstract
Objective: To determine the reproducibility of classifying uterine fibroids using the 2011 International Federation of Gynecology and Obstetrics (FIGO) staging system.
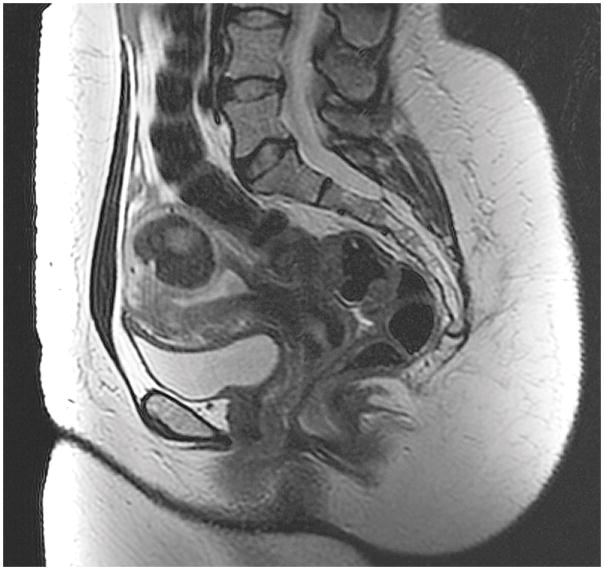
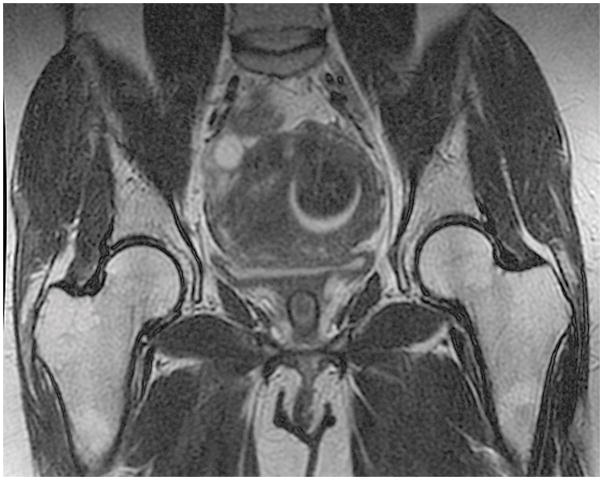
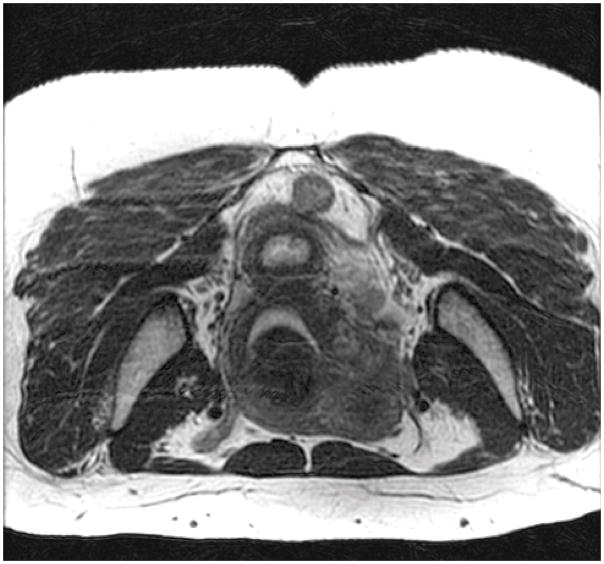
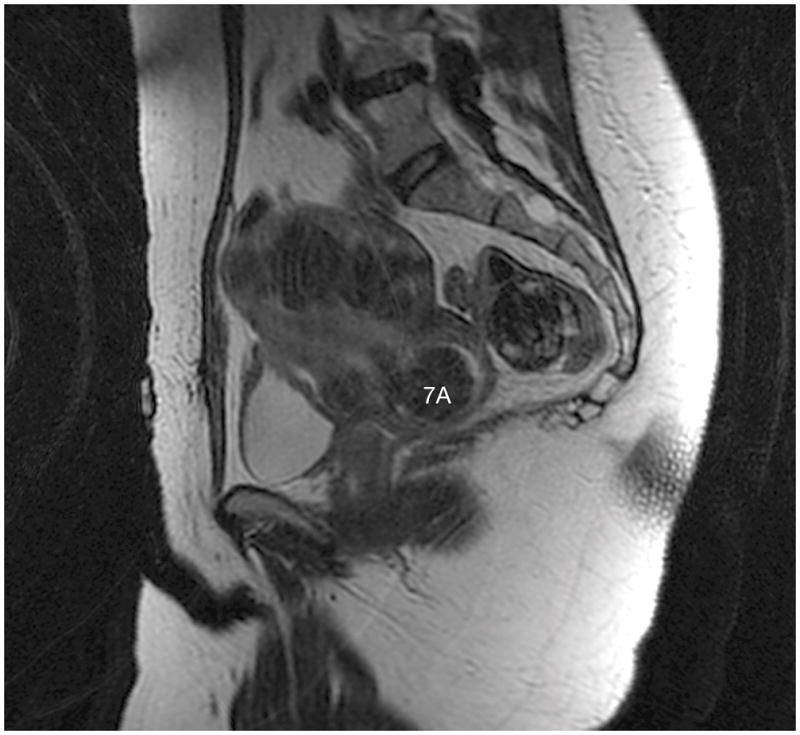
Methods: The present retrospective cohort study included patients presenting for the treatment of symptomatic uterine fibroids at the Gynecology Fibroid Clinic at Mayo Clinic, Rochester, USA, between April 1, 2013 and April 1, 2014. Magnetic resonance imaging of fibroid uteri was performed and the images were independently reviewed by two academic gynecologists and two radiologists specializing in fibroid care. Fibroid classifications assigned by each physician were compared and the significance of the variations was graded by whether they would affect surgical planning.
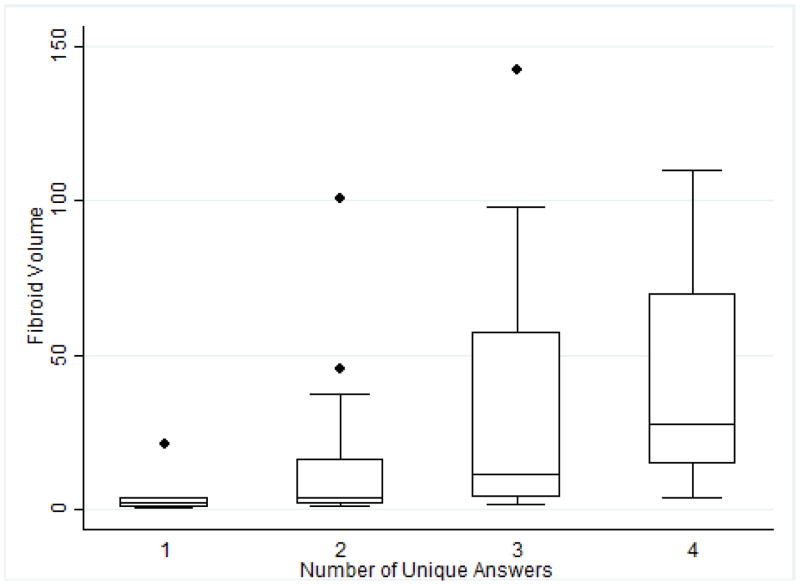
Results: There were 42 fibroids from 23 patients; only 6 (14%) fibroids had unanimous classification agreement. The majority (36 [86%]) had at least two unique answers and 4 (10%) fibroids had four unique classifications. Variations in classification were not associated with physician specialty. More than one-third of the classification discrepancies would have impacted surgical planning.
Conclusion: FIGO fibroid classification was not consistent among four fibroid specialists. The variation was clinically significant for 36% of the fibroids. Additional validation of the FIGO fibroid classification system is needed.
Keywords: FIGO; Abnormal uterine bleeding; Fibroids; Leiomyoma; Myoma; Staging.
© 2017 International Federation of Gynecology and Obstetrics.
Conflict of interest statement
SKL-T has received research funding, paid to the Mayo Clinic, from Truven Health Analytics Inc, and InSightec Ltd (Israel). She is on the data safety monitoring board for the Uterine Leiomyoma (fibroid) Treatment with Radiofrequency Ablation trial (ULTRA trial; Halt Medical, Inc) and has received royalties for UpToDate. GKH has received research funding from InSightec Ltd (Israel). EAS is a consultant for AbbVie, Allergan, Astellas Pharma, Bayer Health Care, Gynesonics, and Viteava, and has received royalties from UpToDate and the Massachusetts Medical Society. The authors have no other conflicts of interest.
Figures


Similar articles
-
The feasibility of high-resolution organ-axial T2-weighted MRI when combined with federation of gynecology and obstetrics (FIGO) classification of uterine fibroid patients.Abdom Radiol (NY). 2025 Aug;50(8):3764-3772. doi: 10.1007/s00261-024-04776-w. Epub 2025 Jan 11. Abdom Radiol (NY). 2025. PMID: 39794535 Free PMC article.
-
Outcome of magnetic resonance-Guided focused ultrasound surgery (MRgFUS) for FIGO class 1 fibroids.Eur J Obstet Gynecol Reprod Biol. 2018 Feb;221:119-122. doi: 10.1016/j.ejogrb.2017.12.025. Epub 2017 Dec 14. Eur J Obstet Gynecol Reprod Biol. 2018. PMID: 29288921
-
Two novel classification systems for uterine fibroids and subsequent uterine reconstruction after myomectomy.Arch Gynecol Obstet. 2017 Mar;295(3):675-680. doi: 10.1007/s00404-016-4268-6. Epub 2016 Dec 20. Arch Gynecol Obstet. 2017. PMID: 28000025
-
Benign and malignant pathology of the uterus.Best Pract Res Clin Obstet Gynaecol. 2018 Jan;46:12-30. doi: 10.1016/j.bpobgyn.2017.10.004. Epub 2017 Oct 16. Best Pract Res Clin Obstet Gynaecol. 2018. PMID: 29126743 Review.
-
MRI-based pictorial review of the FIGO classification system for uterine fibroids.Abdom Radiol (NY). 2021 May;46(5):2146-2155. doi: 10.1007/s00261-020-02882-z. Epub 2021 Jan 1. Abdom Radiol (NY). 2021. PMID: 33385249 Review.
Cited by
-
The feasibility of high-resolution organ-axial T2-weighted MRI when combined with federation of gynecology and obstetrics (FIGO) classification of uterine fibroid patients.Abdom Radiol (NY). 2025 Aug;50(8):3764-3772. doi: 10.1007/s00261-024-04776-w. Epub 2025 Jan 11. Abdom Radiol (NY). 2025. PMID: 39794535 Free PMC article.
-
Clinical comparison of laparoscopic and open surgical approaches for uterus-preserving myomectomy: a retrospective analysis on patient-reported outcome, postoperative morbidity and pregnancy outcomes.Arch Gynecol Obstet. 2025 May;311(5):1359-1369. doi: 10.1007/s00404-024-07818-2. Epub 2024 Nov 27. Arch Gynecol Obstet. 2025. PMID: 39601810 Free PMC article.
-
Endometrial cancer combined with polycystic ovary syndrome in 9 women under 40-years old: A case report.Biomed Rep. 2020 Nov;13(5):50. doi: 10.3892/br.2020.1357. Epub 2020 Sep 9. Biomed Rep. 2020. PMID: 32963779 Free PMC article.
-
Uterine extension determined by MRI: a useful parameter for differentiating subserosal leiomyomas from ovarian tumors.Abdom Radiol (NY). 2022 Mar;47(3):1142-1149. doi: 10.1007/s00261-021-03401-4. Epub 2022 Jan 7. Abdom Radiol (NY). 2022. PMID: 34994842
-
A novel tumor mutational burden-based risk model predicts prognosis and correlates with immune infiltration in ovarian cancer.Front Immunol. 2022 Aug 8;13:943389. doi: 10.3389/fimmu.2022.943389. eCollection 2022. Front Immunol. 2022. PMID: 36003381 Free PMC article.
References
-
- Day Baird D, Dunson DB, Hill MC, Cousins D, Schectman JM. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol. 2003;188(1):100–107. - PubMed
-
- Munro MG, Critchley HO, Fraser IS. The flexible FIGO classification concept for underlying causes of abnormal uterine bleeding. Semin Reprod Med. 2011;29(5):391–399. - PubMed
-
- Munro MG, Critchley HO, Fraser IS. The FIGO classification of causes of abnormal uterine bleeding in the reproductive years. Fertility and Sterility. 2011;95(7):2204–2208. 2208 e2201–2203. - PubMed
-
- Critchley HO, Munro MG, Broder M, Fraser IS. A five-year international review process concerning terminologies, definitions, and related issues around abnormal uterine bleeding. Semin Reprod Med. 2011;29(5):377–382. - PubMed
-
- Wamsteker K, Emanuel MH, de Kruif JH. Transcervical hysteroscopic resection of submucous fibroids for abnormal uterine bleeding: results regarding the degree of intramural extension. Obstet Gynecol. 1993;82(5):736–740. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
