

An efficacy analysis of whole-body magnetic resonance imaging in the diagnosis and follow-up of polymyositis and dermatomyositis
- PMID: 28715432
- PMCID: PMC5513424
- DOI: 10.1371/journal.pone.0181069
An efficacy analysis of whole-body magnetic resonance imaging in the diagnosis and follow-up of polymyositis and dermatomyositis
Abstract
Objectives: To evaluate the value of whole-body magnetic resonance imaging (WBMRI) in diagnosing muscular and extra muscular lesions in patients with polymyositis (PM) and dermatomyositis (DM).
Methods: A retrospective analysis of WBMRI data from PM/DM patients who met the Bohan and Peter diagnostic criteria was performed. X2 test was used to compare the rate of positive diagnosis of newly diagnosed patients using WBMRI, serum creatine kinase test, and EMG. McNemar test was used to compare the performance of WBMRI and chest CT in detecting interstitial lung disease (ILD).
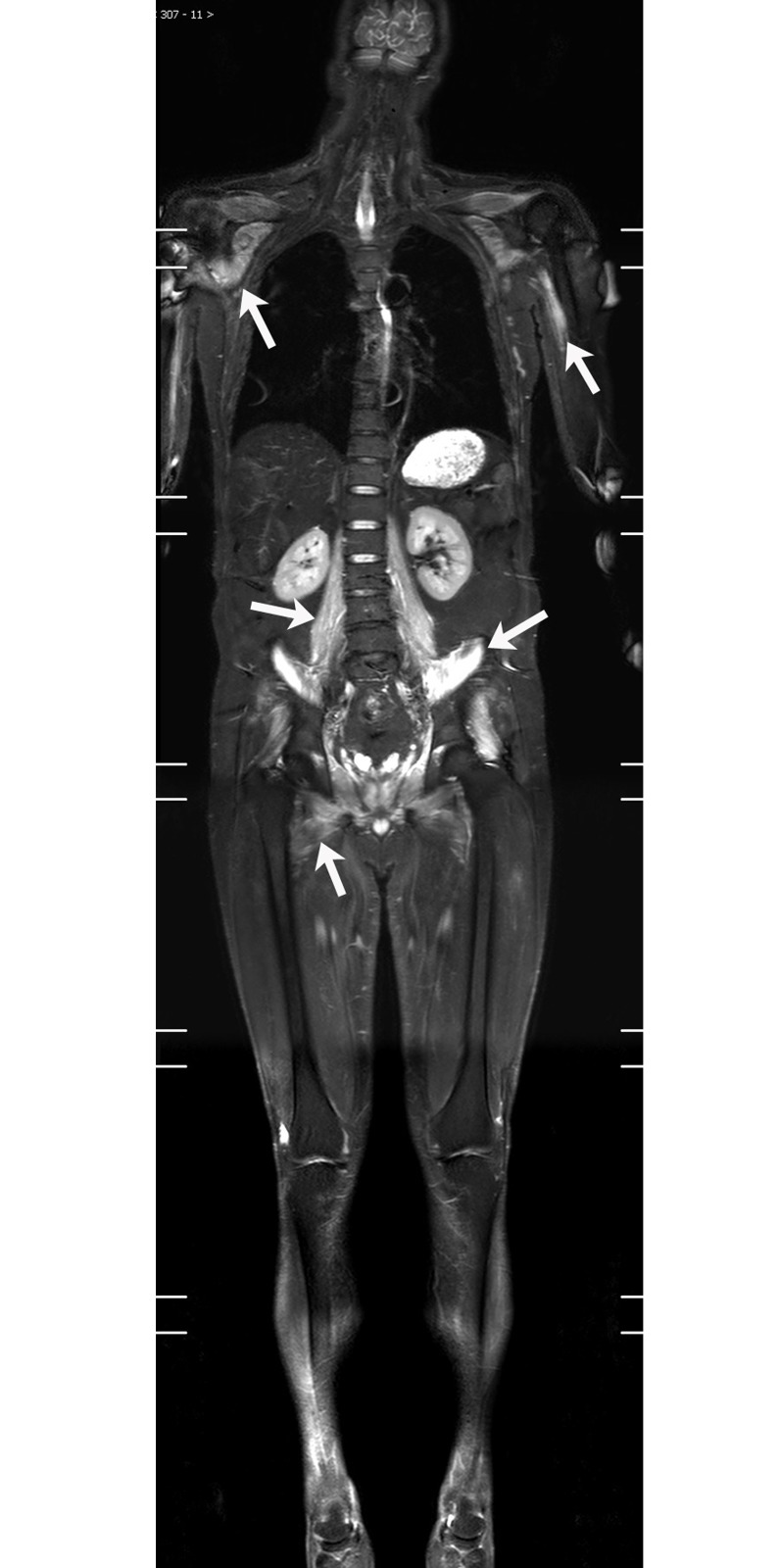
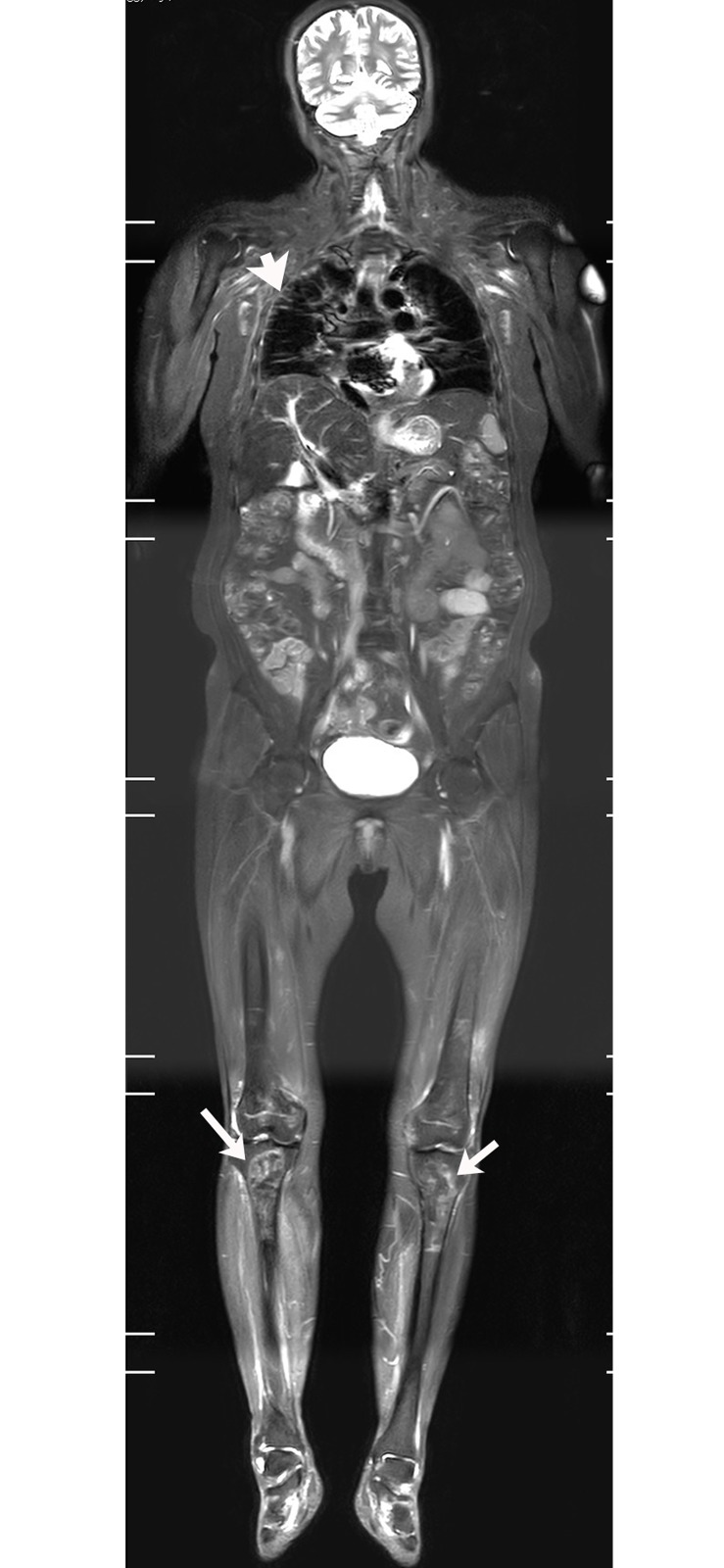
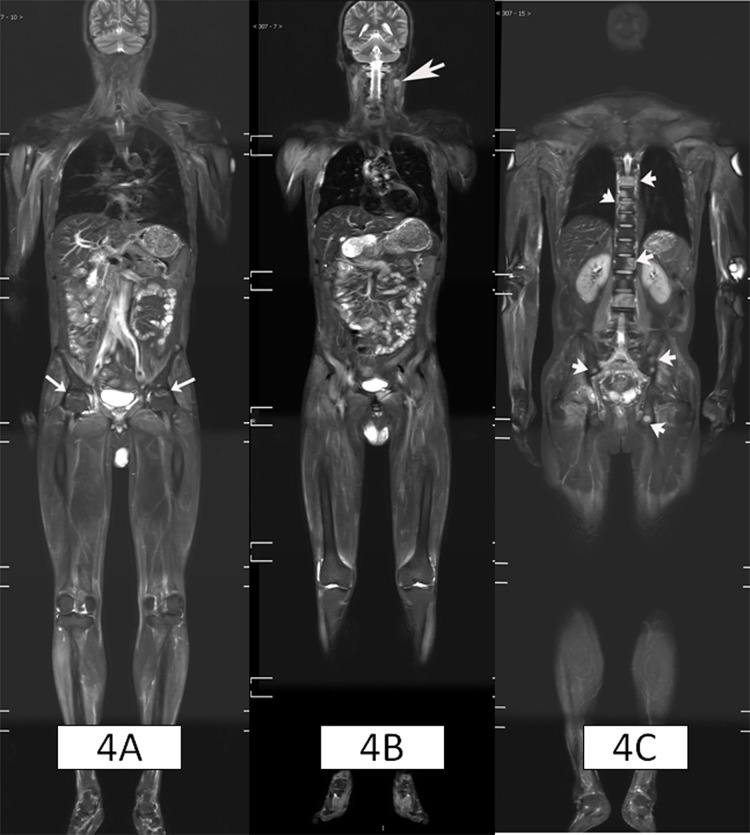
Results: The study included 129 patients (30 PM cases and 99 DM cases). Of them, 81.4% (105/129) showed a visible inflammatory muscular edema on their WBMRI; 29.5% (38/129) had varying degrees of fatty infiltration (9 cases with clear muscular atrophy). Of the 66 newly diagnosed patients, the positive rates of WBMRI, muscle biopsy, serum creatine kinase test and EMG were 86.4% (57/66), 92.4% (61/66), 71.2% (47/66) and 71.1% (32/45), respectively. There was no significant difference in the positive rates between WBMRI and muscle biopsy (X2 = 1.28, P = 0.258). The WBMRI had a higher positive rate than both serum creatine kinase test (X2 = 4.53, P = 0.033) and EMG (X2 = 3.92, P = 0.047). In addition to muscular changes, WBMRI also detected interstitial lung disease (ILD) in 38 cases (29.5%), osteonecrosis in 15 cases (11.6%), and neoplastic lesions (5 malignant; 7 benign) in 12 cases (9.3%). Of the 61 patients who underwent routine chest CT examinations, the WBMRI and CT revealed ILD in 29 cases and 35 cases respectively. There was no significant difference in the sensitivity between WBMRI and CT (p = 0.146).
Conclusions: WBMRI is a sensitive, non-invasive and efficient imaging method. It comprehensively displays the extent of muscular involvement in PM/DM patients, and it has the ability to diagnose other associated extra muscular diseases, such as ILD and systemic malignancy. WBMRI can also help screen steroid-induced osteonecrosis.
Conflict of interest statement
Figures



References
-
- Dalakas MC, Hohlfeld R. Polymyositis and dermatomyositis. Lancet. 2003;362:971–82. doi: 10.1016/S0140-6736(03)14368-1 - DOI - PubMed
-
- Del Grande F, Carrino JA, Del Grande M, Mammen AL, Christopher Stine L. Magnetic resonance imaging of inflammatory myopathies. Top Magn Reson Imaging. 2011;22:39–43. doi: 10.1097/RMR.0b013e31825b2c35 - DOI - PubMed
-
- Tomasová Studynková J, Charvát F, Jarosová K, Vencovsky J. The role of MRI in the assessment of polymyositis and dermatomyositis. Rheumatology (Oxford). 2007;46:1174–9. - PubMed
-
- Connor A, Stebbings S, Anne Hung N, Hammond-Tooke G, Meikle G, Highton J. STIR MRI to direct muscle biopsy in suspected idiopathic inflammatory myopathy. J Clin Rheumatol. 2007;13:341–5. doi: 10.1097/RHU.0b013e31815dca0a - DOI - PubMed
-
- Kuo GP, Carrino JA. Skeletal muscle imaging and inflammatory myopathies. Curr Opin Rheumatol. 2007;19:530–5. doi: 10.1097/BOR.0b013e3282efdc66 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
