

Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and Treatment
- PMID: 28715518
- PMCID: PMC9641643
- DOI: 10.1001/jamapediatrics.2017.1689
Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and Treatment
Erratum in
-
Error in Table.JAMA Pediatr. 2017 Sep 1;171(9):919. doi: 10.1001/jamapediatrics.2017.3169. JAMA Pediatr. 2017. PMID: 28873169 Free PMC article. No abstract available.
Abstract
Importance: Cerebral palsy describes the most common physical disability in childhood and occurs in 1 in 500 live births. Historically, the diagnosis has been made between age 12 and 24 months but now can be made before 6 months' corrected age.
Objectives: To systematically review best available evidence for early, accurate diagnosis of cerebral palsy and to summarize best available evidence about cerebral palsy-specific early intervention that should follow early diagnosis to optimize neuroplasticity and function.
Evidence review: This study systematically searched the literature about early diagnosis of cerebral palsy in MEDLINE (1956-2016), EMBASE (1980-2016), CINAHL (1983-2016), and the Cochrane Library (1988-2016) and by hand searching. Search terms included cerebral palsy, diagnosis, detection, prediction, identification, predictive validity, accuracy, sensitivity, and specificity. The study included systematic reviews with or without meta-analyses, criteria of diagnostic accuracy, and evidence-based clinical guidelines. Findings are reported according to the PRISMA statement, and recommendations are reported according to the Appraisal of Guidelines, Research and Evaluation (AGREE) II instrument.
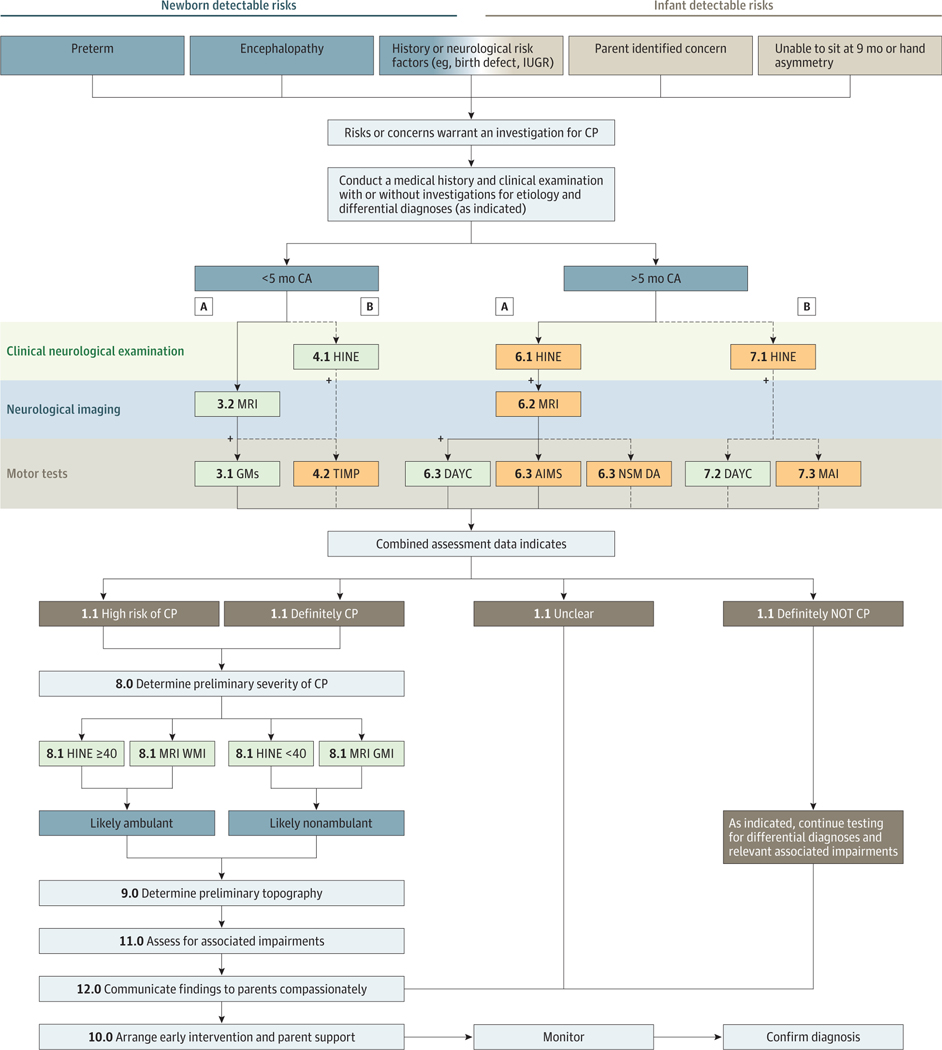
Findings: Six systematic reviews and 2 evidence-based clinical guidelines met inclusion criteria. All included articles had high methodological Quality Assessment of Diagnostic Accuracy Studies (QUADAS) ratings. In infants, clinical signs and symptoms of cerebral palsy emerge and evolve before age 2 years; therefore, a combination of standardized tools should be used to predict risk in conjunction with clinical history. Before 5 months' corrected age, the most predictive tools for detecting risk are term-age magnetic resonance imaging (86%-89% sensitivity), the Prechtl Qualitative Assessment of General Movements (98% sensitivity), and the Hammersmith Infant Neurological Examination (90% sensitivity). After 5 months' corrected age, the most predictive tools for detecting risk are magnetic resonance imaging (86%-89% sensitivity) (where safe and feasible), the Hammersmith Infant Neurological Examination (90% sensitivity), and the Developmental Assessment of Young Children (83% C index). Topography and severity of cerebral palsy are more difficult to ascertain in infancy, and magnetic resonance imaging and the Hammersmith Infant Neurological Examination may be helpful in assisting clinical decisions. In high-income countries, 2 in 3 individuals with cerebral palsy will walk, 3 in 4 will talk, and 1 in 2 will have normal intelligence.
Conclusions and relevance: Early diagnosis begins with a medical history and involves using neuroimaging, standardized neurological, and standardized motor assessments that indicate congruent abnormal findings indicative of cerebral palsy. Clinicians should understand the importance of prompt referral to diagnostic-specific early intervention to optimize infant motor and cognitive plasticity, prevent secondary complications, and enhance caregiver well-being.
Conflict of interest statement
Figures
Comment in
-
Are Structural Magnetic Resonance Imaging and General Movements Assessment Sufficient for Early, Accurate Diagnosis of Cerebral Palsy?JAMA Pediatr. 2018 Feb 1;172(2):198-199. doi: 10.1001/jamapediatrics.2017.4812. JAMA Pediatr. 2018. PMID: 29279893 No abstract available.
-
Are Structural Magnetic Resonance Imaging and General Movements Assessment Sufficient for Early, Accurate Diagnosis of Cerebral Palsy?-Reply.JAMA Pediatr. 2018 Feb 1;172(2):199. doi: 10.1001/jamapediatrics.2017.4815. JAMA Pediatr. 2018. PMID: 29279897 No abstract available.
References
-
- Rosenbaum P, Paneth N, Leviton A, et al. A report: the definition and classification of cerebral palsy April 2006 [published correction appears in Dev Med Child Neurol. 2007;49(6):480]. Dev Med Child Neurol Suppl. 2007;109:8–14. - PubMed
-
- Report of the Australian Cerebral Palsy Register, Birth Years 1993–2009, September 2016. https://www.cpregister.com/pubs/pdf/ACPR-Report_Web_2016.pdf. Accessed 2016. - PubMed
-
- Granild-Jensen JB, Rackauskaite G, Flachs EM, Uldall P. Predictors for early diagnosis of cerebral palsy from national registry data. Dev Med Child Neurol. 2015;57(10):931–935. - PubMed
-
- Hubermann L, Boychuck Z, Shevell M, Majnemer A. Age at referral of children for initial diagnosis of cerebral palsy and rehabilitation: current practices. J Child Neurol. 2016;31(3):364–369. - PubMed
-
- Novak I, Hines M, Goldsmith S, Barclay R. Clinical prognostic messages from a systematic review on cerebral palsy. Pediatrics. 2012;130(5):e1285–e1312. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
