

Epidemiological and clinical profile of paediatric malaria: a cross sectional study performed on febrile children in five epidemiological strata of malaria in Cameroon
- PMID: 28716002
- PMCID: PMC5513087
- DOI: 10.1186/s12879-017-2587-2
Epidemiological and clinical profile of paediatric malaria: a cross sectional study performed on febrile children in five epidemiological strata of malaria in Cameroon
Abstract
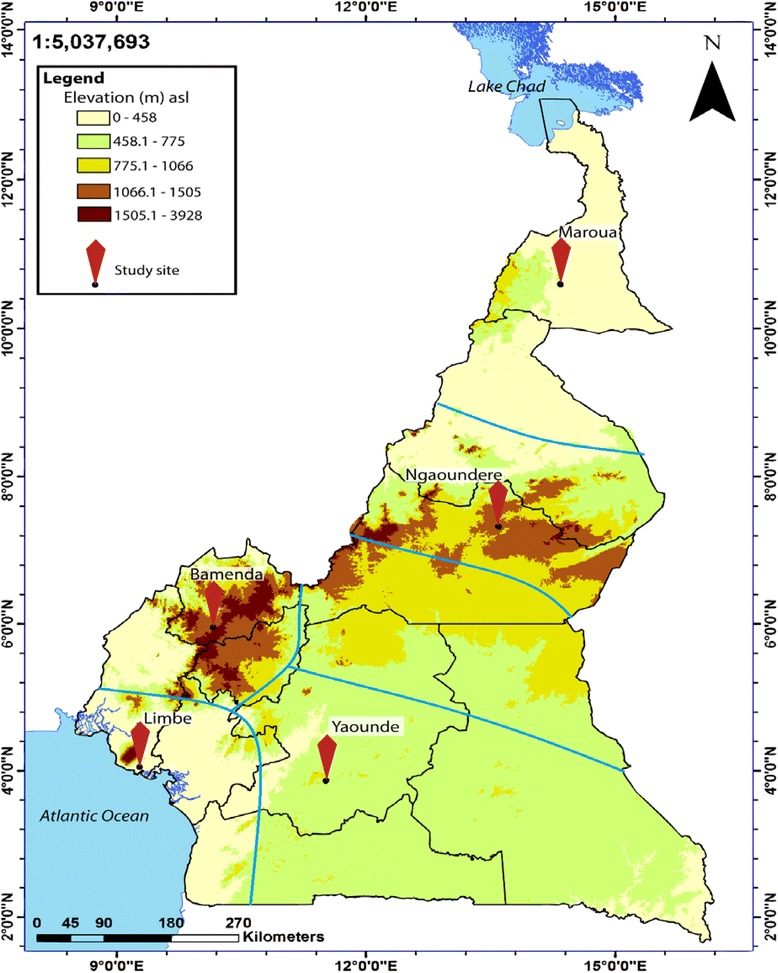
Background: In the wake of a decline in global malaria, it is imperative to describe the epidemiology of malaria in a country to inform control policies. The purpose of this study was to describe the epidemiological and clinical profile of paediatric malaria in five epidemiological strata of malaria in Cameroon including: the Sudano-sahelian (SS) strata, the High inland plateau (HIP) strata, the South Cameroonian Equatorial forest (SCEF) strata, the High western plateau (HWP) strata, and the Coastal (C) strata.
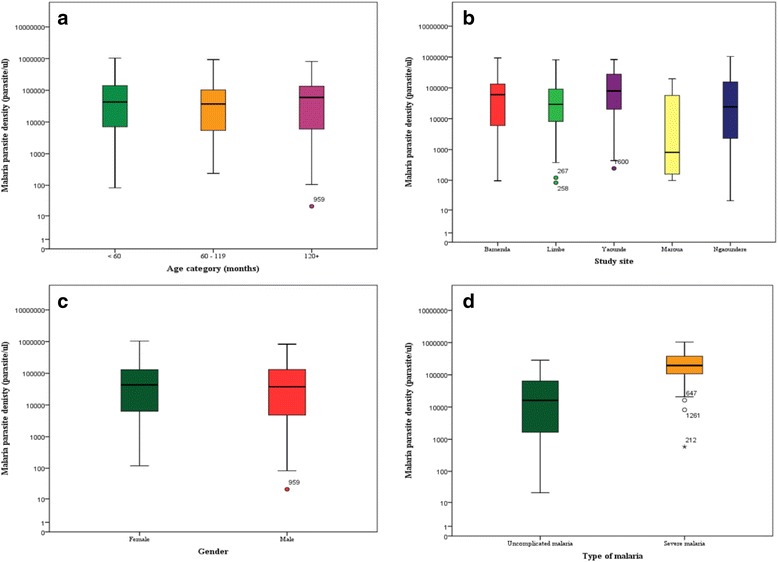
Methods: This study involved 1609 febrile children (≤15 years) recruited using reference hospitals in the five epidemiological strata. Baseline characteristics were determined; blood glucose level was measured by a glucometer, malaria parasitaemia was assessed by Giemsa microscopy, and complete blood count was performed using an automated hematology analyser. Severe malaria was assessed and categorized based on WHO criteria.
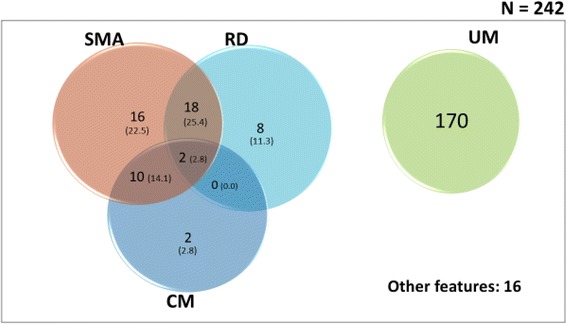
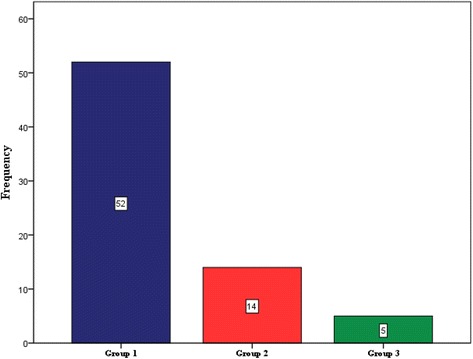
Results: An overall prevalence of 15.0% (95% CI: 13.3-16.9) for malaria was observed in this study. Malaria prevalence was significantly higher in children between 60 and 119 months (p < 0.001) and in Limbe (C strata) (p < 0.001). The overall rate of severe malaria (SM) attack in this study was 29.3%; SM was significantly higher in children below 60 months (p < 0.046). Although not significant, the rate of SM was highest in Maroua (SS strata) and lowest in Limbe in the C strata. The main clinical phenotypes of SM were hyperparasitaemia, severe malaria anaemia and impaired consciousness. The majority (73.2%) of SM cases were in group 1 of the WHO classification of severe malaria (i.e. the most severe form). The malaria case-fatality rate was 5.8%; this was higher in Ngaoundere (HIP strata) (p = 0.034).
Conclusion: In this study, malaria prevalence decreased steadily northward, from the C strata in the South to the SS strata in the North of Cameroon, meanwhile the mortality rate associated with malaria increased in the same direction. On the contrary, the rate of severe malaria attack was similar across the different epidemiological strata. Immunoepidemiological studies will be required to shed more light on the observed trends.
Keywords: Cameroon; Epidemiological strata; Paediatric malaria; Prevalence; Severe malaria; Uncomplicated malaria.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was approved by the National Ethics Committee of Research for Human Health no 2014/12/518/CE/CNERSH/SP. Administrative clearance was obtained from the Directors of the various hospitals used for this study. Written informed consent was obtained from the parents or guardians of the children prior to participation in this study.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Comparative analysis of IgG and IgG subclasses against Plasmodium falciparum MSP-119 in children from five contrasting bioecological zones of Cameroon.Malar J. 2019 Jan 22;18(1):16. doi: 10.1186/s12936-019-2654-9. Malar J. 2019. PMID: 30670064 Free PMC article.
-
Variation in the immune responses against Plasmodium falciparum merozoite surface protein-1 and apical membrane antigen-1 in children residing in the different epidemiological strata of malaria in Cameroon.Malar J. 2017 Nov 9;16(1):453. doi: 10.1186/s12936-017-2105-4. Malar J. 2017. PMID: 29121929 Free PMC article.
-
Identification of the Plasmodium species in clinical samples from children residing in five epidemiological strata of malaria in Cameroon.Trop Med Health. 2017 Jun 15;45:14. doi: 10.1186/s41182-017-0058-5. eCollection 2017. Trop Med Health. 2017. PMID: 28630585 Free PMC article.
-
Malaria parasitaemia, anaemia and malnutrition in children less than 15 years residing in different altitudes along the slope of Mount Cameroon: prevalence, intensity and risk factors.Malar J. 2018 Sep 24;17(1):336. doi: 10.1186/s12936-018-2492-1. Malar J. 2018. PMID: 30249261 Free PMC article.
-
The epidemiology of malaria.Ann Trop Med Parasitol. 1997 Oct;91(7):763-9. doi: 10.1080/00034989760518. Ann Trop Med Parasitol. 1997. PMID: 9625932 Review.
Cited by
-
Comparative analysis of IgG and IgG subclasses against Plasmodium falciparum MSP-119 in children from five contrasting bioecological zones of Cameroon.Malar J. 2019 Jan 22;18(1):16. doi: 10.1186/s12936-019-2654-9. Malar J. 2019. PMID: 30670064 Free PMC article.
-
Evaluating the dual reactivity on SD bioline malaria rapid diagnosis tests as a potential indicator of high parasitemia due to Plasmodium falciparum.Pathog Glob Health. 2021 Oct-Dec;115(7-8):487-495. doi: 10.1080/20477724.2021.1953684. Epub 2021 Jul 26. Pathog Glob Health. 2021. PMID: 34309493 Free PMC article.
-
Malaria and HIV coinfection in sub-Saharan Africa: prevalence, impact, and treatment strategies.Res Rep Trop Med. 2018 Jul 27;9:123-136. doi: 10.2147/RRTM.S154501. eCollection 2018. Res Rep Trop Med. 2018. PMID: 30100779 Free PMC article. Review.
-
Coverage and determinants of Intermittent Preventive Treatment in pregnancy (IPTp) in Cameroon, Guinea, Mali, and Nigeria.PLoS One. 2024 Nov 1;19(11):e0313087. doi: 10.1371/journal.pone.0313087. eCollection 2024. PLoS One. 2024. PMID: 39485743 Free PMC article.
-
User fee exemption and malaria treatment-seeking for children under five in a Cameroonian health district: a cross-sectional study.Malar J. 2023 Apr 13;22(1):124. doi: 10.1186/s12936-023-04509-2. Malar J. 2023. PMID: 37055809 Free PMC article.
References
-
- World Health Organisation . World malaria report 2015. Geneva: World Health Organisation; 2015.
-
- World Health Organisation . World malaria report 2014. Geneva: World Health Organisation; 2014.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
