

The Comprehensive Post-Acute Stroke Services (COMPASS) study: design and methods for a cluster-randomized pragmatic trial
- PMID: 28716014
- PMCID: PMC5513078
- DOI: 10.1186/s12883-017-0907-1
The Comprehensive Post-Acute Stroke Services (COMPASS) study: design and methods for a cluster-randomized pragmatic trial
Abstract
Background: Patients discharged home after stroke face significant challenges managing residual neurological deficits, secondary prevention, and pre-existing chronic conditions. Post-discharge care is often fragmented leading to increased healthcare costs, readmissions, and sub-optimal utilization of rehabilitation and community services. The COMprehensive Post-Acute Stroke Services (COMPASS) Study is an ongoing cluster-randomized pragmatic trial to assess the effectiveness of a comprehensive, evidence-based, post-acute care model on patient-centered outcomes.
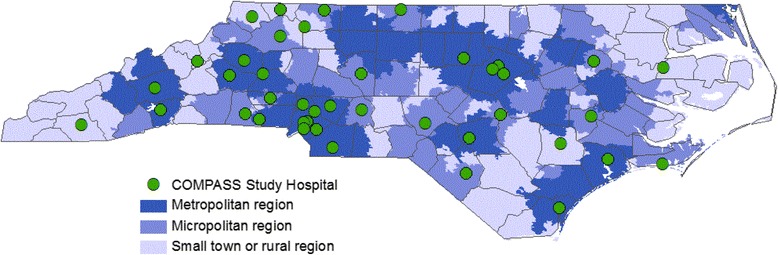
Methods: Forty-one hospitals in North Carolina were randomized (as 40 units) to either implement the COMPASS care model or continue their usual care. The recruitment goal is 6000 patients (3000 per arm). Hospital staff ascertain and enroll patients discharged home with a clinical diagnosis of stroke or transient ischemic attack. Patients discharged from intervention hospitals receive 2-day telephone follow-up; a comprehensive clinic visit within 2 weeks that includes a neurological evaluation, assessments of social and functional determinants of health, and an individualized COMPASS Care Plan™ integrated with a community-specific resource database; and additional follow-up calls at 30 and 60 days post-stroke discharge. This model is consistent with the Centers for Medicare and Medicaid Services transitional care management services provided by physicians or advanced practice providers with support from a nurse to conduct patient assessments and coordinate follow-up services. Patients discharged from usual care hospitals represent the control group and receive the standard of care in place at that hospital. Patient-centered outcomes are collected from telephone surveys administered at 90 days. The primary endpoint is patient-reported functional status as measured by the Stroke Impact Scale 16. Secondary outcomes are: caregiver strain, all-cause readmissions, mortality, healthcare utilization, and medication adherence. The study engages patients, caregivers, and other stakeholders (including policymakers, advocacy groups, payers, and local community coalitions) to advise and support the design, implementation, and sustainability of the COMPASS care model.
Discussion: Given the high societal and economic burden of stroke, identifying a care model to improve recovery, independence, and quality of life is critical for stroke survivors and their caregivers. The pragmatic trial design provides a real-world assessment of the COMPASS care model effectiveness and will facilitate rapid implementation into clinical practice if successful.
Trial registration: Clinicaltrials.gov: NCT02588664 ; October 23, 2015.
Keywords: Functional status; Patient-centered care; Pragmatic trial; Rehabilitation; Stroke; Transitions of care.
Conflict of interest statement
Ethics approval and consent to participate
This research project was reviewed and approved by the Wake Forest University Health Sciences IRB, which acts as a central IRB for 36 participating hospitals. Local IRB review and approval was granted by Cape Fear Valley Medical Center and New Hanover Regional Medical Center. Novant Health Presbyterian Healthcare IRB provided review and approval for the three participating Novant sites. The University of North Carolina at Chapel Hill IRB reviewed all data management and outcomes related activities.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Olson DM, Cox M, Pan W, Sacco RL, Fonarow GC, Zorowitz R, et al. Death and rehospitalization after transient ischemic attack or acute ischemic stroke: one-year outcomes from the adherence evaluation of acute ischemic stroke-longitudinal registry. J Stroke Cerebrovasc Dis. 2013;22:e181–e188. doi: 10.1016/j.jstrokecerebrovasdis.2012.11.001. - DOI - PubMed
-
- Ovbiagele B, Goldstein LB, Higashida RT, Howard VJ, Johnston SC, Khavjou OA, et al. Forecasting the future of stroke in the United States: a policy statement from the American Heart Association and American Stroke Association. Stroke. 2013;44:2361–2375. doi: 10.1161/STR.0b013e31829734f2. - DOI - PubMed
-
- Rosamond W, Johnson A, Bennett P, O'Brien E, Mettam L, Jones S, et al. Monitoring and improving acute stroke care: the North Carolina stroke care Collaborative. N C Med J. 2012;73:494–498. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
