

Cytomegalovirus viraemia and mortality in renal transplant recipients in the era of antiviral prophylaxis. Lessons from the western Australian experience
- PMID: 28716027
- PMCID: PMC5514475
- DOI: 10.1186/s12879-017-2599-y
Cytomegalovirus viraemia and mortality in renal transplant recipients in the era of antiviral prophylaxis. Lessons from the western Australian experience
Abstract
Background: Cytomegalovirus (CMV) establishes a lifelong infection that is efficiently controlled by the immune system; this infection can be reactivated in case of immunosuppression such as following solid organ transplantation. CMV viraemia has been associated with CMV disease, as well as increased mortality and allograft failure. Prophylactic antiviral medication is routinely given to renal transplant recipients, but reactivation during and following cessation of antiviral prophylaxis is known to occur. The aims of this study were to assess the incidence, timing and impact of CMV viraemia in renal transplant recipients and to determine the level of viraemia associated with adverse clinical outcomes.
Methods: Data from all adult (18 years and over) Western Australian renal transplant recipients transplanted between 1 January 2007 and 31 December 2012 were obtained from the Australia and New Zealand Dialysis and Transplant registry and were supplemented with data obtained from clinical records. Potential risk factors for detectable CMV viraemia (≥600 copies/ml) and all-cause mortality were assessed using univariable analysis and Cox Proportional Hazards Regression.
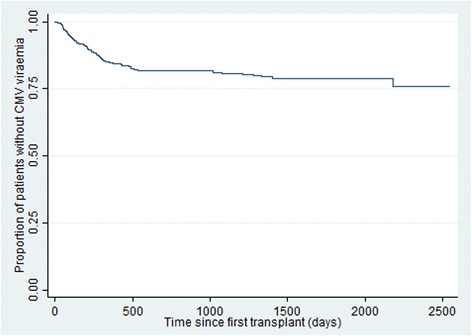
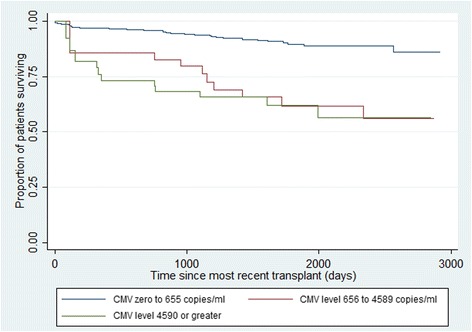
Results: There were 438 transplants performed on 435 recipients. The following factors increased the risk of CMV viraemia with viral loads ≥600 copies/ml: Donor positive/Recipient negative status; receiving a graft from a deceased donor; and receiving a graft from a donor aged 60 years and over. CMV viraemia with viral loads ≥656 copies/ml was a risk factor for death following renal transplantation, as was being aged 65 years and above at transplant, being Aboriginal and having vascular disease. Importantly 37% of the episodes of CMV viraemia with viral loads ≥656 copies/ml occurred while the patients were expected to be on CMV prophylaxis.
Conclusions: CMV viraemia (≥656 copies/ml) was associated with all-cause mortality in multivariable analysis, and CMV viraemia at ≥656 copies/ml commonly occurred during the period when renal transplant recipients were expected to be on antiviral prophylaxis. A greater vigilance in monitoring CMV levels if antiviral prophylaxis is stopped prematurely or poor patient compliance is suspected could protect some renal transplant recipients from adverse outcomes such as premature mortality.
Keywords: Cytomegalovirus reactivation; Mortality; Renal transplantation; Risk factors.
Conflict of interest statement
Ethics approval and consent to participate
Data obtained from the ANZDATA registry included the patient unique medical record number (UMRN) to enable matching with laboratory data and obtaining information from patient charts. After obtaining the additional data, the UMRNs were removed from the record and the ANZDATA patient record number was used as the identifier. Patient consent was not obtained for this study as it was impractical to obtain patient consent and because the risk of adverse outcomes from the study is very low. Approval for the study was obtained from the Sir Charles Gairdner Hospital Human Research Ethics Committee (approval number 2015–022) and from the Curtin University Human Research Ethics Committee (approval number HR64/2015).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
