

Extra-corporeal membrane oxygenation for refractory cardiogenic shock after adult cardiac surgery: a systematic review and meta-analysis
- PMID: 28716039
- PMCID: PMC5512816
- DOI: 10.1186/s13019-017-0618-0
Extra-corporeal membrane oxygenation for refractory cardiogenic shock after adult cardiac surgery: a systematic review and meta-analysis
Abstract
Background: Postcardiotomy cardiogenic shock (PCCS) refractory to inotropic support and intra-aortic balloon pump (IABP) occurs rarely but is almost universally fatal without mechanical circulatory support. In this systematic review and meta-analysis we looked at the evidence behind the use of veno-arterial extra-corporeal membrane oxygenation (VA ECMO) in refractory PCCS from a patient survival rate and determinants of outcome viewpoint.
Methods: A systematic review was performed in January 2017 using PubMed (with no defined time period) using the keywords "postcardiotomy", "cardiogenic shock", "extracorporeal membrane oxygenation" and "cardiac surgery". We excluded papers pertaining to ECMO following paediatric cardiac surgery, medical causes of cardiogenic shock, as well as case reports, review articles, expert opinions, and letters to the editor. Once the studies were collated, a meta-analysis was performed on the proportion of survivors in those papers that met the inclusion criteria. Meta-regression was performed for the most commonly reported adverse prognostic indicators (API).
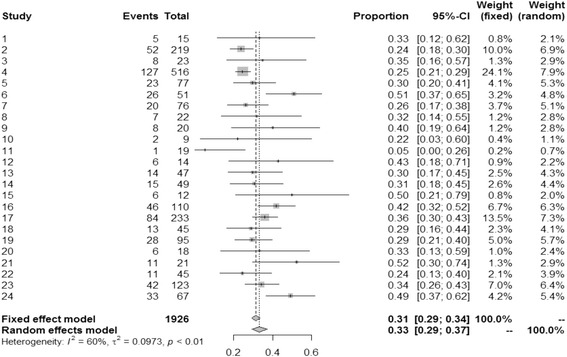
Results: We identified 24 studies and a cumulative pool of 1926 patients from 1992 to 2016. We tabulated the demographic data, including the strengths and weaknesses for each of the studies, outcomes of VA ECMO for refractory PCCS, complications, and APIs. All the studies were retrospective cohort studies. Meta-analysis of the moderately heterogeneous data (95% CI 0.29 to 0.34, p < 0.01, I 2 = 60%) revealed overall survival rate to hospital discharge of 30.8%. Some of the commonly reported APIs were advanced age (>70 years, 95% CI -0.057 to 0.001, P = 0.058), and long ECMO support (95% CI -0.068 to 0.166, P = 0.412). Postoperative renal failure, high EuroSCORE (>20%), diabetes mellitus, obesity, rising lactate whilst on ECMO, gastrointestinal complications had also been reported.
Conclusion: Haemodynamic support with VA ECMO provides a survival benefit with reasonable intermediate and long-term outcomes. Many studies had reported advanced age, renal failure and prolonged VA ECMO support as the most likely APIs for VA ECMO in PCCS. EuroSCORE can be utilized to anticipate the need for prophylactic perioperative VA ECMO in the high-risk category. APIs can be used to aid decision-making regarding both the institution and weaning of ECMO for refractory PCCS.
Keywords: Cardiogenic shock; Extra-corporeal membrane oxygenation; Postcardiotomy.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable as this is a meta-analysis.
Consent for publication
Not applicable as this is a meta-analysis.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Mohite PN, Sabashnikov A, Patil NP, Sáez DG, Zych B, Popov AF, et al. Short-term ventricular assist device in post-cardiotomy cardiogenic shock: factors influencing survival. J Artif Organs. 17(3):228–35. - PubMed
-
- Rastan AJ, Dege A, Mohr M, Doll N, Falk V, Walther T, et al. Early and late outcomes of 517 consecutive adult patients treated with extracorporeal membrane oxygenation for refractory postcardiotomy cardiogenic shock. J Thorac Cardiovasc Surg. 2010;139:302–311. doi: 10.1016/j.jtcvs.2009.10.043. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
