

Clinical workflow for MR-only simulation and planning in prostate
- PMID: 28716090
- PMCID: PMC5513123
- DOI: 10.1186/s13014-017-0854-4
Clinical workflow for MR-only simulation and planning in prostate
Abstract
Purpose: To describe the details and experience of implementing a MR-only workflow in the clinic for simulation and planning of prostate cancer patients.
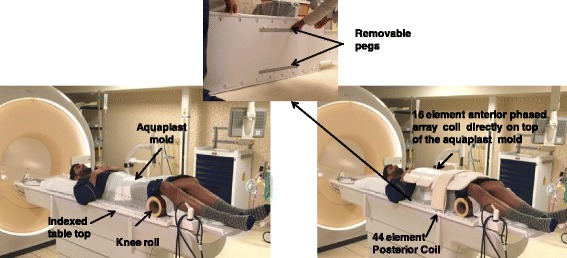
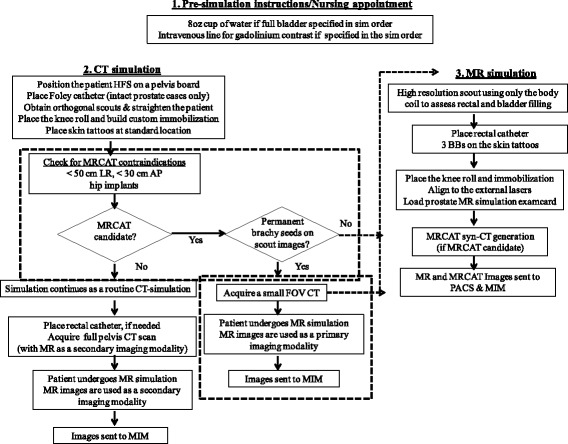
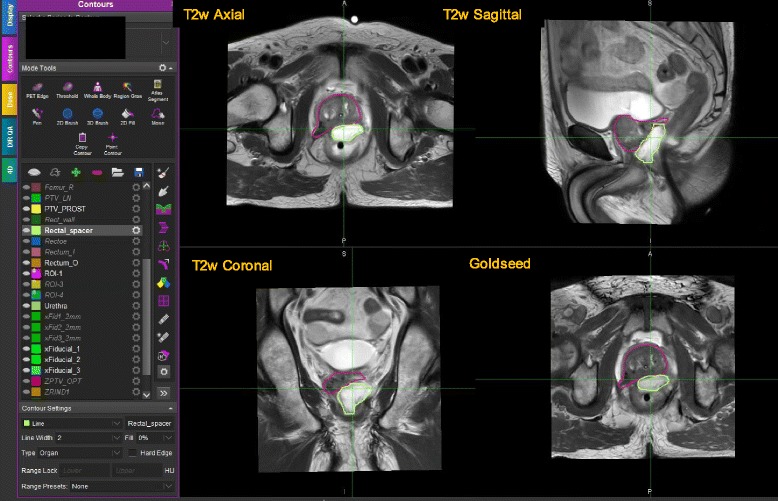
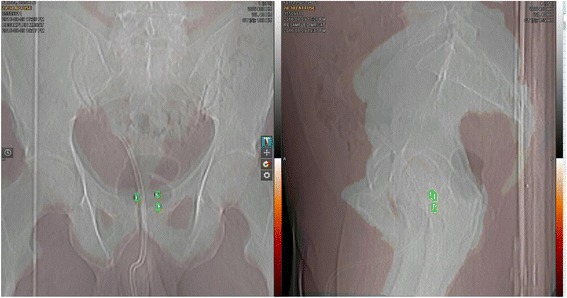
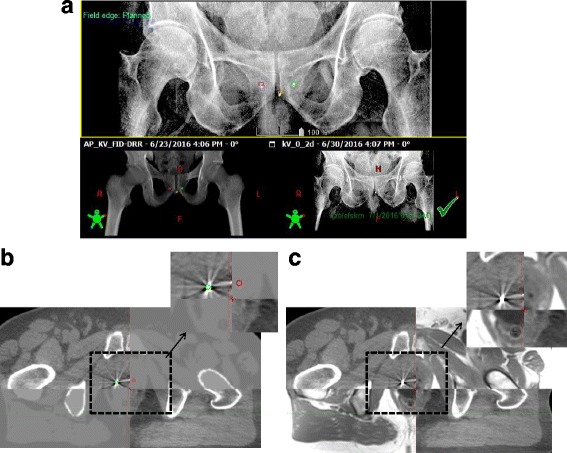
Methods: Forty-eight prostate cancer patients from June 2016 - Dec 2016 receiving external beam radiotherapy were scheduled to undergo MR-only simulation. MR images were acquired for contouring (T2w axial, coronal, sagittal), synthetic-CT generation (3D FFE-based) and fiducial identification (3D bFFE-based). The total acquisition time was 25 min. Syn-CT was generated at the console using commercial software called MRCAT. As part of acceptance testing of the MRCAT package, external laser positioning system QA (< 2 mm) and geometric fidelity QA (< 2 mm within 50 cm LR and 30 cm AP) were performed and baseline values were set. Our current combined CT + MR simulation process was modified to accommodate a MRCAT-based MR-only simulation workflow. An automated step-by-step process using a MIM™ workflow was created for contouring on the MR images. Patient setup for treatment was achieved by matching the MRCAT DRRs with the orthogonal KV radiographs based on either fiducial ROIs or bones. 3-D CBCTs were acquired and compared with the MR/syn-CT to assess the rectum and bladder filling compared to simulation conditions.
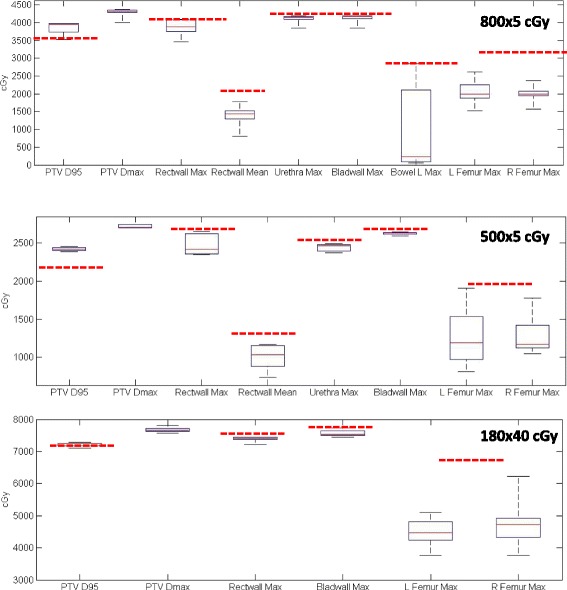
Results: Forty-two patients successfully underwent MR-only simulation and met all of our institutional dosimetric objectives that were developed based on a CT + MR-based workflow. The remaining six patients either had a hip prosthesis or their large body size fell outside of the geometric fidelity QA criteria and thus they were not candidates for MR-only simulation. A total time saving of ~15 min was achieved with MR-based simulation as compared to CT + MR-based simulation. An automated and organized MIM workflow made contouring on MR much easier, quicker and more accurate compared with combined CT + MR images because the temporal variations in normal structure was minimal. 2D and 3D treatment setup localization based on bones/fiducials using a MRCAT reference image was successfully achieved for all cases.
Conclusions: MR-only simulation and planning with equivalent or superior target delineation, planning and treatment setup localization accuracy is feasible in a clinical setting. Future work will focus on implementing a robust 3D isotropic acquisition for contouring.
Keywords: Clinical workflow; MRCAT; Prostate cancer; Synthetic CT.
Conflict of interest statement
Ethics approval and consent to participate
The study was conducted under MSKCC IRB approved retrospective protocol number 16-682 and 16-1309.
Consent for publication
Written informed consent for publication of their picture used in Fig. 1 was obtained from the volunteer. A copy of the consent form is available for review by the editor.
Competing interests
The authors declare that they have no competing interests.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
