

Visumax femtolasik versus Moria M2 microkeratome in mild to moderate myopia: efficacy, safety, predictability, aberrometric changes and flap thickness predictability
- PMID: 28716114
- PMCID: PMC5512974
- DOI: 10.1186/s12886-017-0520-5
Visumax femtolasik versus Moria M2 microkeratome in mild to moderate myopia: efficacy, safety, predictability, aberrometric changes and flap thickness predictability
Abstract
Introduction: This is an interventional prospective clinical study which was conducted to evaluate the efficacy, safety, predictability, ocular aberrations, and flap thickness predictability of Visumax femtosecond laser (FSL) compared to Moria M2 microkeratome (MK) in mild to moderate myopia.
Methods: This study included 60 eyes who were divided into two groups. Thirty eyes in group (I) in which the flap was created with Visumax FSL, while in group II (30 eyes) the Moria M2 MK was used. Keratometric, refractive, and aberrometric measurements were compared preoperatively and 3 months postoperatively. The intraoperative subtraction pachymetry (the SP 100 Handy pachymeter (Tomey, Nagoya, Japan) was used for preoperative pachymetry and flap thickness measurement.
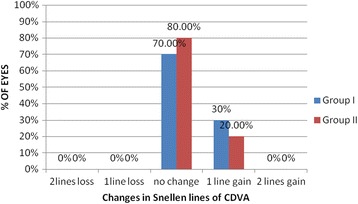
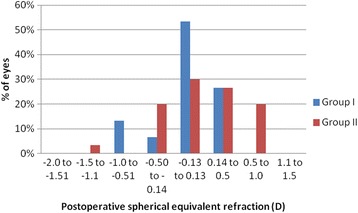
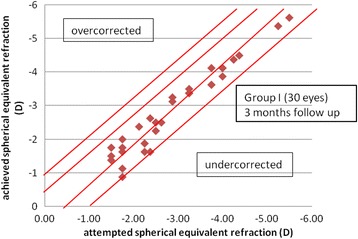
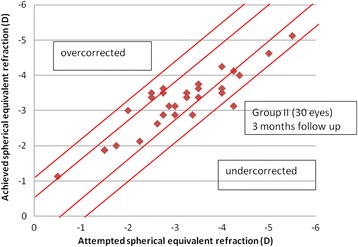
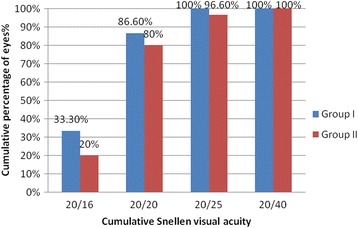
Results: No significant difference was found between the two groups in regards to postoperative manifest sphere, spherical equivalent, astigmatism, safety indices nor ocular aberrations. Twenty six eyes (86.6%) in group I and 23 eyes in group II (76.6%) were within ±0.5D of the intended correction and 23 eyes (76.6%) in group I and 15 eyes in group II (50%) were within ±0.25D of the intended correction. In group I, the mean postoperative actual flap thickness was 100.12 ± 16.1 μm (81 to 122 μm), while in group II, it was 104.6 ± 20.1 μm (62 to 155 μm). The difference was statistically significant (p = 0.001).
Conclusions: Both Visumax and Moria M2 MK are safe and effective in treating myopia with no statistically significant difference in induction of ocular aberrations but with potential advantage for Visumax regarding predictability. More accurate flap thickness is achieved with Visumax femtolasik.
Trial registration: This study was retrospectively registered on 19/6/2017. Trial registration number NCT03193411 , clinicalTrials.gov .
Keywords: Moria 2; Visumax; myopia.
Conflict of interest statement
Ethics approval and consent to participate
This is a clinical study, and the research was approved by the local Institutional Review Board of the Dar Alshifa Hospital, Kuwait and conducted according to the tenets of the Declaration of Helsinki. Written informed consent to participate was obtained for each subject prior to the study.
Consent for publication
Not applicable for this study.
Competing interests
The authors declare that they have no competing interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Rosa AM, Neto Murta J, Quadrado MJ, Tavares C, Lobo C, Van Velze R, Castanheira-Dinis A. FSL versus mechanical MKs for flap creation in laser in situ keratomileusis and effect of postoperative measurement interval on estimated femtosecond flap thickness. J Cataract Refract Surg. 2009;35:833–838. doi: 10.1016/j.jcrs.2008.12.038. - DOI - PubMed
-
- Kurtz RM, Horvath C, Liu HH, Krueger RR, Juhasz T. Lamellar refractive surgery with scanned infrastromal picosecond and FSL pulses in animal eyes. J Refract Surg. 1998;14:541–548. - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
