

A patient-safety and professional perspective on non-conveyance in ambulance care: a systematic review
- PMID: 28716132
- PMCID: PMC5513207
- DOI: 10.1186/s13049-017-0409-6
A patient-safety and professional perspective on non-conveyance in ambulance care: a systematic review
Abstract
Background: This systematic review aimed to describe non-conveyance in ambulance care from patient-safety and ambulance professional perspectives. The review specifically focussed at describing (1) ambulance non-conveyance rates, (2) characteristics of non-conveyed patients, (3) follow-up care after non-conveyance, (4) existing guidelines or protocols, and (5) influencing factors during the non-conveyance decision making process.
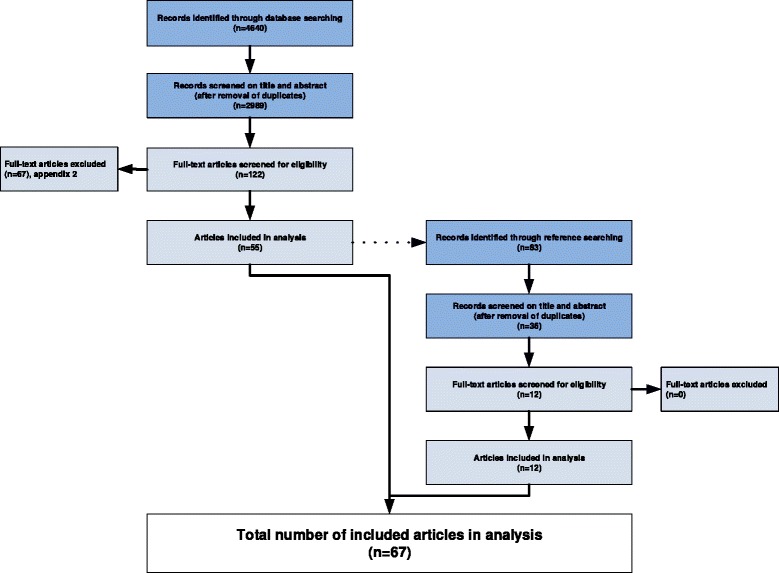
Methods: We systematically searched MEDLINE, PubMed, CINAHL, EMBASE, and reference lists of included articles, in June 2016. We included all types of peer-reviewed designs on the five topics. Couples of two independent reviewers performed the selection process, the quality assessment, and data extraction.
Results: We included 67 studies with low to moderate quality. Non-conveyance rates for general patient populations ranged from 3.7%-93.7%. Non-conveyed patients have a variety of initial complaints, common initial complaints are related to trauma and neurology. Furthermore, vulnerable patients groups as children and elderly are more represented in the non-conveyance population. Within 24 h-48 h after non-conveyance, 2.5%-6.1% of the patients have EMS representations, and 4.6-19.0% present themselves at the ED. Mortality rates vary from 0.2%-3.5% after 24 h, up to 0.3%-6.1% after 72 h. Criteria to guide non-conveyance decisions are vital signs, ingestion of drugs/alcohol, and level of consciousness. A limited amount of non-conveyance guidelines or protocols is available for general and specific patient populations. Factors influencing the non-conveyance decision are related to the professional (competencies, experience, intuition), the patient (health status, refusal, wishes and best interest), the healthcare system (access to general practitioner/other healthcare facilities/patient information), and supportive tools (online medical control, high risk card).
Conclusions: Non-conveyance rates for general and specific patient populations vary. Patients in the non-conveyance population present themselves with a variety of initial complaints and conditions, common initial complaints or conditions are related to trauma and neurology. After non-conveyance, a proportion of patients re-enters the emergency healthcare system within 2 days. For ambulance professionals the non-conveyance decision-making process is complex and multifactorial. Competencies needed to perform non-conveyance are marginally described, and there is a limited amount of supportive tools is available for general and specific non-conveyance populations. This may compromise patient-safety.
Keywords: Clinical competence [MeSH]; Emergency medical services [MeSH]; Non-conveyance; Patient safety [MeSH].
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
