

Detection, risk factors, and functional consequences of cerebral microinfarcts
- PMID: 28716371
- PMCID: PMC5861500
- DOI: 10.1016/S1474-4422(17)30196-5
Detection, risk factors, and functional consequences of cerebral microinfarcts
Abstract
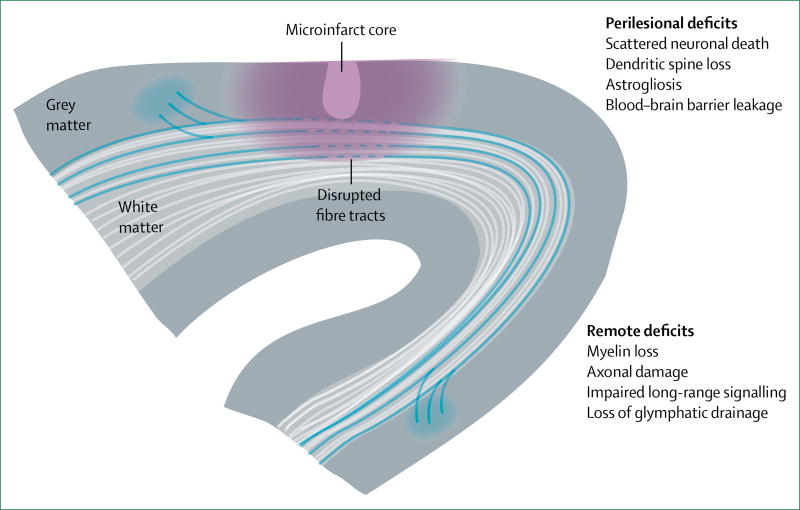
Cerebral microinfarcts are small lesions that are presumed to be ischaemic. Despite the small size of these lesions, affected individuals can have hundreds to thousands of cerebral microinfarcts, which cause measurable disruption to structural brain connections, and are associated with dementia that is independent of Alzheimer's disease pathology or larger infarcts (ie, lacunar infarcts, and large cortical and non-lacunar subcortical infarcts). Substantial progress has been made with regard to understanding risk factors and functional consequences of cerebral microinfarcts, partly driven by new in-vivo detection methods and the development of animal models that closely mimic multiple aspects of cerebral microinfarcts in human beings. Evidence from these advances suggests that cerebral microinfarcts can be manifestations of both small vessel and large vessel disease, that cerebral microinfarcts are independently associated with cognitive impairment, and that these lesions are likely to cause damage to brain structure and function that extends beyond their actual lesion boundaries. Criteria for the identification of cerebral microinfarcts with in-vivo MRI are provided to support further studies of the association between these lesions and cerebrovascular disease and dementia.
Copyright © 2017 Elsevier Ltd. All rights reserved.
Figures
References
-
- Sonnen JA, Larson EB, Crane PK, et al. Pathological correlates of dementia in a longitudinal, population-based sample of aging. Ann Neurol. 2007;62:406–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
