

Emphysematous pyelonephritis: Changing trend of clinical spectrum, pathogenesis, management and outcome
- PMID: 28717547
- PMCID: PMC5503442
- DOI: 10.5152/tud.2016.14227
Emphysematous pyelonephritis: Changing trend of clinical spectrum, pathogenesis, management and outcome
Abstract
Objective: To highlight changing trend of clinical spectrum, comparing management options and predictors of outcome of emphysematous pyelonephritis.
Material and methods: This study included patients who were diagnosed as emphysematous pyelonephritis between August, 2001 to July, 2015. We excluded other possible causes of gas in renal system. Baseline patient characteristics, clinical spectrum, serum and urinary biochemical parameters, radiological findings, management and outcomes were recorded. Patients were classified as "responders" and "non-responders".
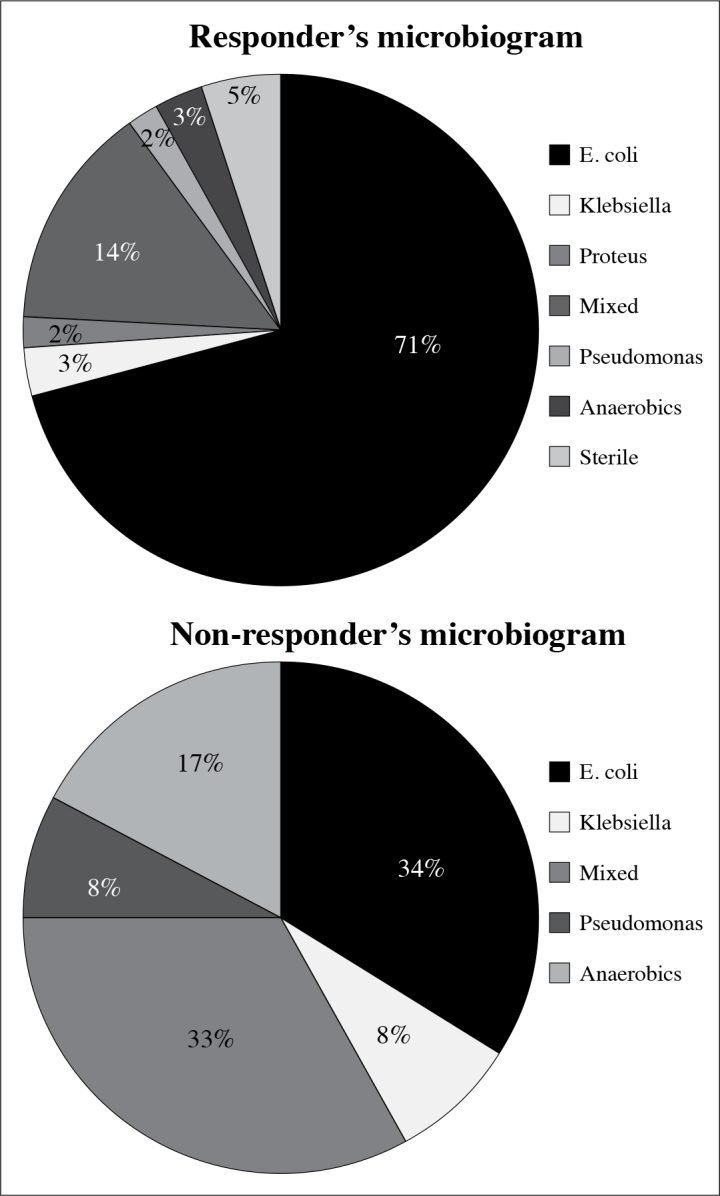
Results: We studied a total of 74 patients and categorised them as responders (62 patients) and non-responders (12 patients). Women outnumbered men constituting 62.16% of the study population (M: F; 1: 1.6). Fever was the most common presenting symptom followed by flank pain. Diabetes mellitus (85.14%) was the most common comorbidity followed by urolithiasis (32.43%). Escherichia coli was the commonest organism grown in urine culture (79.73%). Non-responders had distinct laboratory findings relative to responders as low hemoglobin (7.8±2.1/11.2±3.2 g/dL; p=0.0007), thrombocytopenia (91.67% vs. 11.29%; p=0.0001), proteinuria >3 g/L (50% vs. 6.45%; p=0.0008) and positive blood culture (100% vs. 67.74%; p=0.0288).
Conclusion: Advanced age, higher body mass index, renal impairment, thrombocytopenia, altered sensorium, shock at presentation can be used as scores for poor prognosis. Emphysematous pyelonephritis management requires multidisciplinary collaboration including hydration and electrolyte management, broad spectrum antibiotics, strict glycaemic control, effective urinary drainage and lastly it may require emergency nephrectomy as a salvage procedure.
Keywords: Antibiotics; diabetes mellitus; emphysematous pyelonephritis; upper urinary tract infection.
Conflict of interest statement
Conflict of Interest: No conflict of interest was declared by the authors.
Figures


References
-
- Michaeli J, Mogle P, Perlberg S, Hemiman S, Caine M. Emphysematous pyelonephritis. J Urol. 1984;131:203–8. - PubMed
-
- Wan YL, Lee TY, Bullard MJ, Tsai CC. Acute gas-producing bacterial renal infection: correlation between imaging findings and clinical outcome. Radiology. 1996;198:433–8. https://doi.org/10.1148/radiology.198.2.8596845. - DOI - PubMed
-
- Godec CJ, Cass AS, Berkseth R. Emphysematous pyelonephritis in a solitary kidney. J Urol. 1980;124:119–21. - PubMed
-
- DePauw AP, Ross G., Jr Emphysematous pyelonephritis in a solitary kidney. J Urol. 1981;125:734–46. - PubMed
-
- Hudson MA, Weyman PJ, van der Vliet AH, Catalona WJ. Emphysematous pyelonephritis: successful management by percutaneous drainage. J Urol. 1986;136:884–6. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources